Download
1 / 1
10 likes | 66 Views
3. Brain activity for evoked knee pain. INTRODUCTION.

E N D
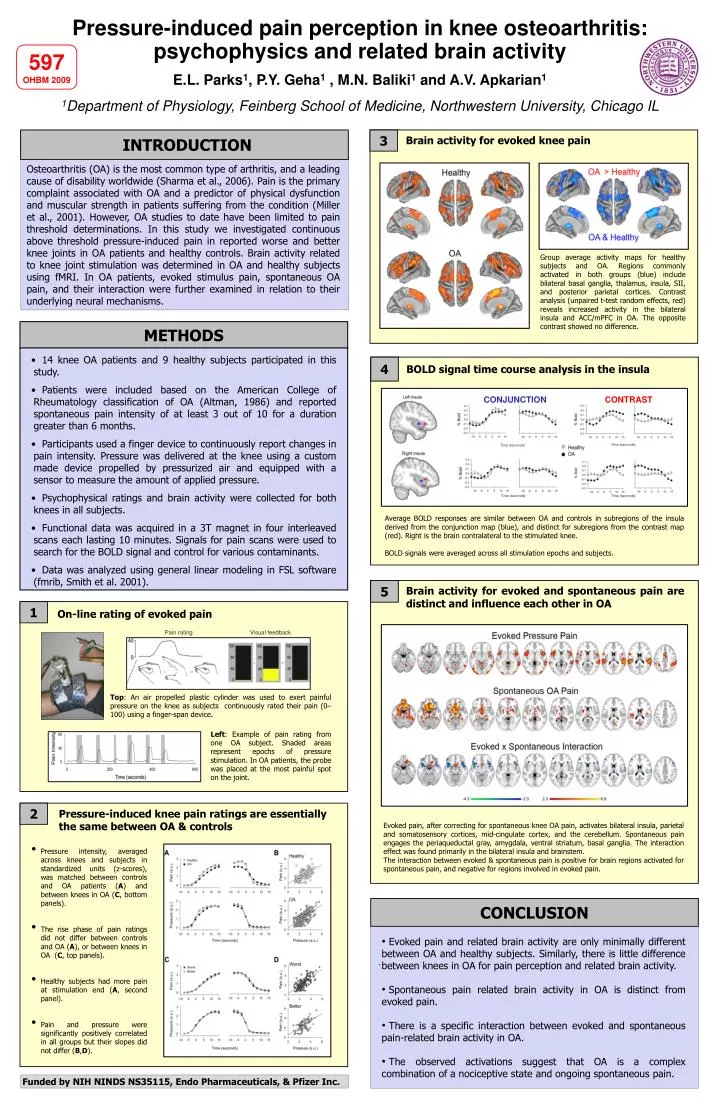
3 Brain activity for evoked knee pain INTRODUCTION Osteoarthritis (OA) is the most common type of arthritis, and a leading cause of disability worldwide (Sharma et al., 2006). Pain is the primary complaint associated with OA and a predictor of physical dysfunction and muscular strength in patients suffering from the condition (Miller et al., 2001). However, OA studies to date have been limited to pain threshold determinations. In this study we investigated continuous above threshold pressure-induced pain in reported worse and better knee joints in OA patients and healthy controls. Brain activity related to knee joint stimulation was determined in OA and healthy subjects using fMRI. In OA patients, evoked stimulus pain, spontaneous OA pain, and their interaction were further examined in relation to their underlying neural mechanisms. METHODS • 14 knee OA patients and 9 healthy subjects participated in this study. • Patients were included based on the American College of Rheumatology classification of OA (Altman, 1986) and reported spontaneous pain intensity of at least 3 out of 10 for a duration greater than 6 months. • Participants used a finger device to continuously report changes in pain intensity. Pressure was delivered at the knee using a custom made device propelled by pressurized air and equipped with a sensor to measure the amount of applied pressure. • Psychophysical ratings and brain activity were collected for both knees in all subjects. • Functional data was acquired in a 3T magnet in four interleaved scans each lasting 10 minutes. Signals for pain scans were used to search for the BOLD signal and control for various contaminants. • Data was analyzed using general linear modeling in FSL software (fmrib, Smith et al. 2001). 4 BOLD signal time course analysis in the insula R S2 (56 -26 18) CONCLUSION Pressure-induced pain perception in knee osteoarthritis: psychophysics and related brain activity 597 OHBM 2009 E.L. Parks1, P.Y. Geha1 , M.N. Baliki1 and A.V. Apkarian1 1Department of Physiology, Feinberg School of Medicine, Northwestern University, Chicago IL Group average activity maps for healthy subjects and OA. Regions commonly activated in both groups (blue) include bilateral basal ganglia, thalamus, insula, SII, and posterior parietal cortices. Contrast analysis (unpaired t-test random effects, red) reveals increased activity in the bilateral insula and ACC/mPFC in OA. The opposite contrast showed no difference. CONJUNCTION CONTRAST Time (seconds) Time (seconds) Time (seconds) Time (seconds) Average BOLD responses are similar between OA and controls in subregions of the insula derived from the conjunction map (blue), and distinct for subregions from the contrast map (red). Right is the brain contralateral to the stimulated knee. BOLD signals were averaged across all stimulation epochs and subjects. Brain activity for evoked and spontaneous pain are distinct and influence each other in OA 1 On-line rating of evoked pain 5 Pain rating Visual feedback Top: An air propelled plastic cylinder was used to exert painful pressure on the knee as subjects continuously rated their pain (0–100) using a finger-span device. Left: Example of pain rating from one OA subject. Shaded areas represent epochs of pressure stimulation. In OA patients, the probe was placed at the most painful spot on the joint. Pressure-induced knee pain ratings are essentially the same between OA & controls 2 Evoked pain, after correcting for spontaneous knee OA pain, activates bilateral insula, parietal and somatosensory cortices, mid-cingulate cortex, and the cerebellum. Spontaneous pain engages the periaqueductal gray, amygdala, ventral striatum, basal ganglia. The interaction effect was found primarily in the bilateral insula and brainstem. The interaction between evoked & spontaneous pain is positive for brain regions activated for spontaneous pain, and negative for regions involved in evoked pain. • Pressure intensity, averaged across knees and subjects in standardized units (z-scores), was matched between controls and OA patients (A) and between knees in OA (C, bottom panels). • The rise phase of pain ratings did not differ between controls and OA (A), or between knees in OA (C, top panels). • Healthy subjects had more pain at stimulation end (A, second panel). • Pain and pressure were significantly positively correlated in all groups but their slopes did not differ (B,D). • Evoked pain and related brain activity are only minimally different between OA and healthy subjects. Similarly, there is little difference between knees in OA for pain perception and related brain activity. • Spontaneous pain related brain activity in OA is distinct from evoked pain. • There is a specific interaction between evoked and spontaneous pain-related brain activity in OA. • The observed activations suggest that OA is a complex combination of a nociceptive state and ongoing spontaneous pain. . Funded by NIH NINDS NS35115, Endo Pharmaceuticals, & Pfizer Inc.