Download
1 / 30
660 likes | 1.66k Views
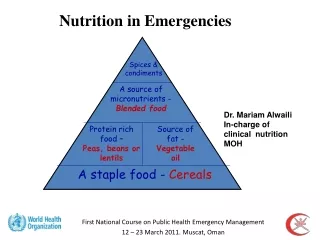
Nutrition in Emergencies . Marie McGrath, Emergency Nutrition Network. Emergency Nutrition Network (ENN). Set up in 1996 by humanitarian agencies To develop sectoral memory and learn from experiences in emergency nutrition and food security Field Exchange www.ennonline.net. Terminology.

E N D
Nutrition in Emergencies Marie McGrath, Emergency Nutrition Network
Emergency Nutrition Network (ENN) • Set up in 1996 by humanitarian agencies • To develop sectoral memory and learn from experiences in emergency nutrition and food security • Field Exchange • www.ennonline.net
Terminology Underweight Stunting Marasmus Micronutrient deficiencies Wasting Kwashiorkor Under-nutrition Over-nutrition Micronutrients Macronutrients
Importance of nutrition in emergencies • Biafran war (1967-1970) • 1 million civilians died • Ethiopian famines 1980s • Mobilised aid Tumultuous scenes at food distribution sites in Ethiopia. Ken Bailey, Field Exchange 12, 2001
Why is nutrition in emergencies important? • Protection of nutritional status in emergencies humanitarian right (international law) • Acutely malnourished - more sick • Sick more likely to get malnourished • Emergencies impact on range of factors – increase risk of malnutrition, illness (morbidity) and death (mortality)
Malnutrition and risk of illness and death • Not infectious disease……. implicated in half child deaths in the world • Some emergencies result in very high levels of severe malnutrition • ‘Cut-offs’ for severe malnutrition is threshold where mortality risk rises sharply • Risk of death of malnourished associated with disease patterns – malaria, diarrhoea, measles, ARI, HIV and AIDS • Nutritional status also affected by reduced food intake due to worsening food security • Relationship between malnutrition and mortality is complicated • Other factors affect mortality • Important to interpret mortality data with nutrition and health information • Crude Mortality Rate (CMR): <1.0/10,000 individuals/day • Under-five Mortality Rate (U5MR): <2.0/10,000 U5s/day
South Sudan, 1998 • U5MR rose faster than CMR. • July, outbreak of dysentery and CMR caught up with U5MR. • July nutrition survey: 80% acute malnutrition (WH <-2 zscores). • October nutrition survey: 48% acute malnutrition, partially explaining continued high mortality despite dysentery under control.
What are the causes of malnutrition? • Immediate causes….individual • Underlying……..households/communities • Basic….society • UNICEF conceptual framework to determine causes of malnutrition
Broad-based approaches to tackle malnutrition • Not just lack of food – complex mix of factors • Interventions to ‘cure’ individuals and prevent death • Interventions to ‘prevent’ malnutrition rates rising • Heath, healthy environment • Ensuring food security (ability of household to access food) • Public nutrition approach
What is an emergency? • Extraordinary-urgent-sudden • Emergency – disaster – crisis An unforseen and often sudden event that causes great damage, destruction and human suffering, CRED, 2007 • Complex – major humanitarian crisis, multi-causal, essentially political nature, system wide response needed • ‘Loud’ v ‘silent’ • Impartiality - basis of and in proportion to need????? MSF ‘top ten’ under-reported • Violence in Central Africa Republic • TB deaths on increase • Conflict in Chechnya • Conflict in Sri Lanka • ……. In 2006, the ‘top ten’ accounted for 7.2 minutes out of 14,512 minutes on three major US TV network nightly newscasts. Five of the countries never mentioned at all.
What is a nutrition emergency? • Classification systems • Severity using acute MN as an indicator of distress • UN-SCN thresholds (1995) • ODI (2003) • FSAU/FAO Integrated food security phase classification (2006) • Howe and Devereux Famine Magnitude Scale 2004 (6 ‘stages’) • Food security (CME<0.2/10,000/d and wasting <2.3%) • Food crisis conditions (CMR>=0.5 but<1/10,000/d and/or wasting >=10% but <20% and/or oedema) • Extreme famine conditions (CMR>=15/10,000/d) • When to respond? • Thresholds for emergency interventions: ODI and FSAU • SMART – reliable and consistent data and reporting
Where do emergencies occur? • Largest famines (excess deaths) in Asia • China 1958-1962, 30 million people died • North Korea, 3.5 million people • Most nutritional emergencies chronic and ‘invisible’ • Allocation of food aid not just wasting: 2000-2004: emergency food aid went to just 6 countries: Ethiopia, Sudan, Afghanistan, Angola, Iraq, North Korea
What are the causes? • Emergencies where acute malnutrition rates rise are usually directly caused by severe shortages of food combined with disease epidemics. • Vulnerability • Poverty, chronic food insecurity, poor infrastructure……………..developing countries • HIV and AIDS • Majority of humanitarian crisis in countries where rates already high • Emergencies can increase the risk of infection, eg rape and sexual explotation in conflict areas • Affects agricultural production (labour loss), intensifies poverty (assets stripped) • No clear associations between malnutrition rates and HIV and AIDS at population level • Climate change • Average global temperatures rising, other ecological changes…increase nutrition emergencies and famine? • Climate vulnerability analysis into frameworks
Triggers for nutrition emergencies • Natural disasters • floods, hurricanes • Droughts develop more slowly • Earthquakes large mortality, less dramatic effect on food security • Conflict • War ‘tactics’ can block access to food/health services • Destroy infrastructure, food production • Political crisis and economic shocks • Zimbabwe • Drought, floods, disruption of farming activities due to political strife, national mismanagement of grain reserves….vulnerability • Individual vulnerability may be linked to social or political status
Who most nutritionally vulnerable in emergencies? • Physiological • U2’s, pregnant and lactating, elderly • Geographical • Political • Internal displacement and refugees • Around 9.2 million refugees and 25 million IDPs worldwide
Increased deaths (mortality) Daily deaths per 10,000 people in selected refugee situations 1998 and 1999 IFE 1/1 AND because infants and children are the most vulnerable... people of all ages children under 5 years Deaths/10,000/Day Camp location Refugee Nutrition Information System, ACC/SCN at WHO, Geneva
Risks of death highest for the youngest at therapeutic feeding centres in Afghanistan, 1999 IFE 1/2 Deaths as % of admissions Age (months) Golden M. Comment on including infants in nutrition surveys: experiences of ACF in Kabul City. Field Exchange 2000;9:16-17
Risk of death higher for malnourished children Distribution of 12.2 million deaths among children under 5 years old in all developing countries, 1995 WHO Geneva, 1995 IFE 1/3
What types of malnutrition occur in emergencies? • Acute malnutrition (wasting), especially in young children • Measured as weight-for-height/presence of bilateral oedema • Moderate acute (MAM): WH>=70%-<80% WH or >=-3 - <-2 z score • Severe acute (SAM): WH<70% or <-3 z score • U5 acute MN as proxy • Micronutrient deficiencies • Clinical, sub-clinical • Dietary diversity • Chronic malnutrition (stunting) • Inhibits full mental and physical potential • Small mothers have small babies
Marasmus(‘wasting malnutrition’) • Severe form acute malnutrition • Generally wasted • Thin arms • Thin face, “old man” • Ribs visible • Sunken eyes • Lack of skin turgor • May be alert but irritable
Kwashiorkor Severe form of acute MN Clinical signs include oedema (bilateral foot oedema, can spread to other parts of body) Cracked and peeling skin, changes in hair colour and texture, lethargy and misery
Micronutrient deficiencies • Iron deficiency (anaemia) • Vitamin A deficiency (xeropthalmia) • Iodine deficiency • Vitamin C deficiency • Niacin deficiency (pellagra) • Thiamine deficiency (beri-beri) • Riboflavin deficiency (ariboflavinosis) Haemacue survey in Tanzania, Field Exchange, Issue 28, July 2006
Source: UNHCR Source: A Seal, Field Exchange 32, Ethiopia, 2004
Micronutrient deficiencies Signs of scurvy: blackness of the legs indicative of haemorrhage. Northern Afghanistan, Field Exchange 13, 2001 Pellagra (niacin deficiency), Angola Field Exchange 30, Angola, 2007
Nutrition Assessment • Establish prevalence of malnutrition • 30x30 cluster • Identify potential causes • Decide on appropriate interventions • Rapid assessment • Nutrition surveys • Nutritional surveillance ACF coverage survey, Uganda, Field Exchange 34, 2008
Nutrition Response in emergencies • Curative, eg therapeutic care • Preventative, eg improving water supply and sanitation to prevent disease epidemics • Food and non-food interventions