Download
1 / 31
310 likes | 399 Views
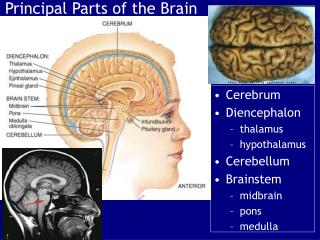
Detecting and Managing Symptom Exaggeration in ‘Brain’ Disorders . Dr Susan Shaw Neuropsychologist PsyD cns@wave.co.nz. Most commonly seen in these ‘Brain’ Disorders. Mild Traumatic Brain Injury Post Concussion Syndrome Chronic Pain Syndromes Chronic Fatigue

E N D
Detecting and Managing Symptom Exaggeration in ‘Brain’ Disorders Dr Susan Shaw Neuropsychologist PsyD cns@wave.co.nz
Most commonly seen in these ‘Brain’ Disorders Mild Traumatic Brain Injury Post Concussion Syndrome Chronic Pain Syndromes Chronic Fatigue Depression / anxiety/PTSD / mental health. Disorders which are ‘high on symptoms – low on signs’
Step 1. Is the progression consistent with expectation? Some disorders improve with time, while others get worse. In order to know if the disorder is progressing in accordance with expectations based on medical literature, you need to know a little bit about what those expectations are. Progressive Vs non-progressive
Non-Progressive • CVA or Stroke – Usually acute event followed by recovery • Considered stable at about 18 months post CVA • Need to look at causes for CVA to determine if the person at risk of another. • Haemorrhagic or ischaemic?
Haemorrhagic or ischaemic • Haemorrhagic usually has low risk for repeat event if caused by a congenital malformation or berry aneurysm, trauma to head. • High blood pressure? – more likely to happen again if cause not treated. • Ischaemic can be due to cholesterol or ‘bubbles’ or ‘clots’. More likely to happen again if cause not treated.
Progressive Some tumours Dementias = Alzheimer’s Disease, Fronto-temporal dementia, Picks Disease, Diffuse Lewy Body Disease. Vascular Dementia Multi Infarct Dementia Mental Health problems like depression – can fluctuate in accordance with psychosocial stressors. Epilepsy can be caused by an acquired injury or can be idiopathic. Not usually progressive if well managed with medication.
General rule Illness / Disease is likely to be progressive Acute injury like trauma, CVA is more likely to recover to some extent and then become stable. Give it at least 18 months.
Detection of Symptom Exaggeration – In the Office Step 1. – Is the course consistent with expectation? Step 2. – Refer for an assessment with a suitably experienced neuropsychologist who will administer psychometric measures to get an objective measurement – not a psychiatrist or a clinical psychologist who will rely on ‘intuition’ as they are wrong 50% of the time!
Detection Fairly easy for neuropsychologists in cases of cognitive symptom exaggeration. Use psychometric measures with robust statistical properties 80 - 90% can be achieved by individuals with severe TBI, advanced dementia and intellectual disability. MTBI client achieving 60% is suspicious!
‘Malingering’ • Slick et al (1999) developed criteria for diagnosing malingering with regard to cognitive and pain disorders. • Key features are as follows: • Inconsistency between reported symptoms and those expected given the documented or reported injury. • Inconsistency between patterns of recovery and those expected given the documented or reported injury. • Inconsistency between performances on cognitive tests and those expected in the context of the injury • Identifiable secondary gain • Failure on tests of symptom validity.
Sensitivity = 0.542 Specificity = 1.00 • Laribee 2003 – atypical patterns of performance on three measures used as indicators of symptom validity = specificity of 1.00. • Does not matter which measures are used • Newer measures of Symptom Validity have better statistical properties, so two measures should suffice.
Robust Evidence If you find that the client meets the Slick et al (1999) criteria for malingering and….. The client fails three measures of symptom validity (e.g.Laribee) … I would argue that this is an extremely strong indication that the test performances were not a valid reflection of the true abilities.
Intervention Avoid confrontation and subsequent defensive behaviour – worsens symptoms. Give a ‘face saving way out’. Help significant others understand the true nature of the problem where it fits with ‘face saving’. Give incentive to ‘recover’
From the very start you can…. Build a good foundation from which to progress rehabilitation. Focus on ensuring the client knows someone understands their condition – generates confidence. Non-progressive - reassure client that recovery is the most likely outcome (expected).
Recovery ‘unknown’ myth Clients often tell me the literature is very non-specific about recovery timeframes, and no-one knows why. ‘Dr Google’ Not true. ‘Narrow’ literature search to be specific to the client e.g. age, gender, health status, mental health history, personality, coping mechanisms, psychosocial supports. Reinforce notion that psychological factors inhibit recovery.
Client expectations predict recovery Whittaker, R. Kemp, S. House, A. Illness perceptions and outcome in mild head injury: a longtitudional study. Journal of Neurology, Neurosurgery and Psychiatry. 2007; 78:644 – 6. Poor outcome predicted by expectation of non-recovery, non-attribution of symptoms to psychological factors and being in receipt of health related benefits at time of initial consultation.
In the Clinic Ascertain Symptom Exaggeration Vs another undiagnosed problem. Determine reasons for Symptom Exaggeration Do something about it – this is the hardest part but is much easier if you have done the first two steps well. Intuition, absent, ‘harden up’ approach – not good
What often happens 1. Detection through ‘Intuition 2. Ascertaining reasons for behaviour is absent 3. Problem managed by confrontation and telling the client to ‘harden up’. This approach does not work!
Case Example 35 year old male Transport business owner 10 employees ‘Hard man’ – very ‘macho’ environment. ‘Hard’ on employees when they made mistakes. High level athlete – determined.
TBI rugby – LOC > 3 mins, nil retro, PTA < 30 mins. Now 1 year post Wife RTW after 12 months maternity leave Wife developed depression Client irritable and unpleasant at home and at work – exacerbated by fatigue. Client had to ‘step in’ at home when wife unwell and care for children aged 1 and 3.
Adamant that RTW was main goal Adamant that recovery period ‘unknown’ but possibly 2 years. No financial incentive for not RTW ‘Failure’ regarding GRTW – stalled. Referred to me ‘Failure’ on SV measures. Strong indicators of cognitive symptom exaggeration. WHY?
At Work Loss of confidence with regard to ability to ‘dominate’ at work following ‘mistake’. Vulnerable Catastrophic thinking with regard to memory. Feeling ‘vindicated’ or ‘Blameless’ if ‘mistake’ due to ‘brain damage’. Acceptable (not my fault) but also very scary (future?)
At Home Resentful that wife ‘stealing thunder’ by having a diagnosis of her own Resentful at having to ‘step in’ and help out when wife unwell, as he was also not feeling the best. Rapid deconditioning from inactivity – concerns about ‘weakness’ in sporting arena.
Combination Resentment Loss of confidence – catastrophic thinking Shifting ‘blame’ Significant physiological changes ? Opting out – ‘driven’ lifestyle – stress – pressure to perform at work, at home and sports field.
What to do? Consider depression Find a ‘face saving’ way out Exercise programme - education Don’t back into a corner or he will come out ‘fighting’ and symptoms will be exaggerated. Wife could be ‘key’.
Neuropsychologist spoke about models of memory to explain ‘mistake’ and reduce catastrophic thinking. Psychologist met with OT to discuss above issues – same page Psychologist met with client to ‘touch’ on some of the above, asking questions and letting client ‘work it out’ himself.
OT reassured client that now a ‘change in tactic’ was to take place. Shift focus from ‘fatigue management’ to confidence building and increased physical strength and fitness OT reassured client that this ‘new’ approach works very well with clients like him. OT reassured client that if TBI related sx would resolve with this approach – those which did not resolve unlikely to be due to TBI
Outcome Wife understood loss of confidence issues and felt greater empathy for him, rather than feeling resentful and frustrated. Improved relationship led to improved mood for both. Wife more able to ‘pull her weight’ at home
Outcome ctd Wife ‘ignored’ complaints of fatigue and headaches, irritable behaviour. Wife praised desirable behaviours and rewarded with ‘extra’ time for gym etc. Client increased fitness gradually and focussed on an ‘event’. RTW took care of itself!
Main points ‘Set the scene’ early on – reassure that most likely outcome is recovery. ‘Counter’ claims of extended recovery by recommending a more ‘narrow’ literature search. Introduce the importance of psychological and personality factors early on.
4 Easy Steps Objective measurement of symptom validity. Determine reasons why Give a ‘face saving’ way out Give incentives to recover and deterrent for non-recovery. Don’t be confrontational!! It makes symptoms worse.