Download
1 / 34
340 likes | 1.48k Views
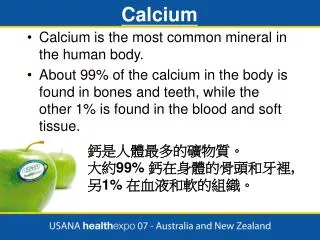
Plasma calcium concentration. mg/dL meq/L mmolL % total Free ionized 5.0 2.5 1.25 50 Protein-bound 4.2 2.1 1.05 44 Complexed 0.8 0.4 0.2 6 Total 10 5.0 2.50 100.

E N D
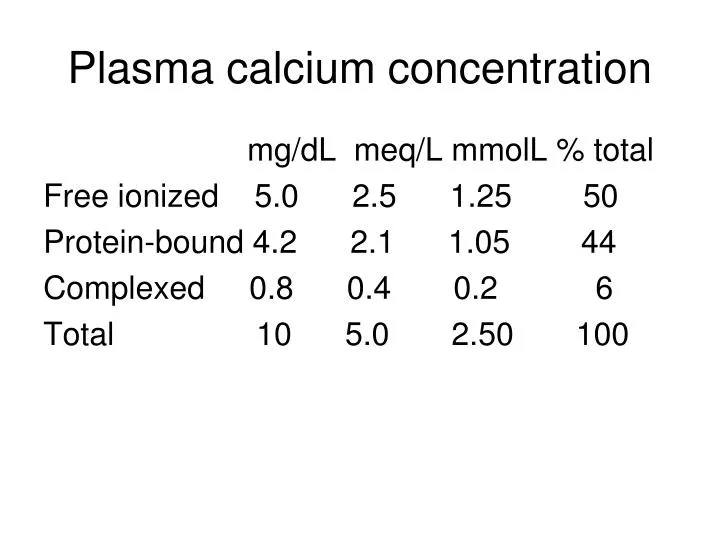
Plasma calcium concentration mg/dL meq/L mmolL % total Free ionized 5.0 2.5 1.25 50 Protein-bound 4.2 2.1 1.05 44 Complexed 0.8 0.4 0.2 6 Total 10 5.0 2.50 100
Serum Ca corrections • Correction of total serum Ca for serum albumin – add 0.8 meq/L for each 1 gm reduction in albumin • Ionized Ca – can obtain if do not have a serum albumin measurement • Gadolinium – certain gadolinium salts can dramatically transiently lower measured total serum Ca
Hypocalcemia – effects of change in serum pH • Alkalosis – decreases ionized Ca • Acidosis – increases ionized Ca • Clinical ramifications - if patient is acidotic and hypocalcemic treatment with NaHCO3 without addressing the hypocalcemia can further lower ionized Ca
Hypocalcemia – signs and symptoms • Weakness • Paresthesias • Seizures • Latent tetany – Trousseau, Chvostek signs • Hypotension • Long QT
Tests for latent tetany • Chvostek sign - tap the skin over the facial nerve in front of the external auditory meatus, causes an ipsilateral contraction of the facial muscles, but up to 10% of population have a positive test • Trousseau sign – inflate BP cuff on arm to 20 mmHg>systolic BP for 3-5 min & watch for carpopedal spasm, insensitive test
Mechanisms of hypocalcemia • Reduced GI absorption – GI disease, hypoparathyroidism, vitamin D deficiency • Renal loss – low Mg, genetic disorders, drugs (e.g. cisplatinum, cyclosporine, aminoglycosides, proton pump inhibitors) • Redistribution of Ca into: bone (post parathyroidectomy) or abdominal cavity (pancreatitis) • Binding by citrate (transfusions) or PO4 load (IV or enema)
Hypocalcemia in critical illness • Mechanisms: low Mg renal failure blood transfusions (citrate) multiple mechanisms in gram negative sepsis including probable cytokine induction of hypoparathyroidism and vitamin D deficiency or resistance • No proof correction of Ca affects course
Hypocalcemia – indications for IV Ca • Patients who are severely symptomatic – tetany, carpopedal spasm, decreased cardiac function, or prolonged QT interval • Asymptomatic patients with an acute decrease if corrected total serum Ca<7.5 mg/dl • Not an indication - neuromuscular irritability such as paresthesias and corrected total serum Ca >7.5; initial treatment with oral Ca sufficient
Hypocalcemia treatment with bolus intravenous Ca • Calcium gluconate – 10 mL of a 10% solution is 90 mg of elemental Ca • Calcium chloride – 10 mL of a 10% solution is 270 mg of elemental Ca • Tissue necrosis with extravasation – much more common with calcium chloride • Code cart – contains Ca chloride • Formation of insoluble Ca salts – occurs when HCO3 or PO4 is added to solution containing Ca • Hyperkalemia with marked EKG changes (with no hypocalcemia) – affects conduction not serum [K+]
Hypocalcemia Rx with Ca infusion • Since duration of action of IV Ca bolus is just 1-3 hours to maintain the serum Ca level may need to give IV infusion • Add 11 amps of Ca gluconate to either D5W or NS to make a 1 L solution with a Ca concentration of 1 mg/ml • Usual starting rate 1 ml/minute or 60 mg/hour of elemental Ca
Hypocalcemia with concurrent hypomagnesemia • Often cannot correct the Ca unless the Mg is corrected • Give 2 gm of Mg (16 meq) of MgSO4 as a 10% solution over 10 to 20 minutes • Followed by 1 gm MgSO4 (8 meq) at 100 mL/hr • Continue intravenous MgSO4 as long as Mg < 1 mg/dL • Careful monitoring if patient has impaired renal function
Vitamin D nomenclature • Vitamin D – cholecalciferol D3, ergocalciferol D2 • 25-hydroxy vitamin D - calcidiol D3, ercalcidiol D2 • Vitamin D receptor agonist - calcitriol D3 (Rocaltrol), paricalcitol D2 (Zemplar) a synthetic analog, doxercalciferol D2 (Hectoral) a synthetic prohormone
Measurement of vitamin D deficiency or insufficiency • Vitamin D deficiency best determined by measuring 25-OH vitamin D even though the active form is 1,25 dihydroxy vitamin D • This is because 1,25 dihydroxy vitamin D levels are often normal in vitamin D insufficiency because of a compensatory increase of PTH which then stimulates conversion of 25 to 1,25 dihydroxy vit D • 25-hydroxy vitamin D levels are reported as a combination of D2 and D3 • Vitamin D deficiency < 20 ng/ml • Vitamin D insufficiency 20-30 ng/ml
Sources of vitamin D • Very few foods contain vitamin D (livers of fatty fish are the exception) • Synthesis in the skin of vitamin D3 during exposure to UV rays in sunlight is a major source • This system is exceedingly efficient and brief casual exposure such as 10-15 minutes of the arms and face is equivalent to ingestion of 200 IU per day • Disabled persons and elderly may have inadequate sun exposure • Skin of those >70 does not convert vitamin D effectively • At northern latitudes there is not enough radiation to convert vitamin D, particularly during the winter
Vitamin D deficiency • Elderly – up to 74% deficient in vitamin D even if adequate intake; suggested guidelines in elderly 800-1000 IU/day • NHANES study – 42% of African American women were deficient vs 4% Caucasian • Response to bisphosphonates – may be blunted if vitamin D deficient
Hypocalcemia – rationale for Rx with calcitriol (Rocaltrol) • PTH stimulates the conversion of 25-hydroxy vitamin D to 1-25 dihydroxy vitamin D • So if give a patient with hypoparathyroidism vitamin D it would not be converted to the active form 1-25 dihydroxy vitamin D (calcitriol) • Calcitriol must be given in this circumstance. • Onset of action – much quicker in onset than vitamin D which may take several days • Offset of action – much quicker than vitamin D, so if develop hypercalcemia of shorter duration • Dosage - start with .25 ug bid, up to 2 ug per day • Elevated urinary Ca and nephrolithiasis – can be induced by calcitriol even if no hypercalcemia
Ergocalciferol vs cholecalciferol • Vitamin D2 – ergocalciferol (nephrologists use since listed in their guidelines) • Vitamin D3 - cholecalciferol, longer half-life, greater activity
Vitamin D dosage in Rx of chronic hypocalcemia Simple dietary deficiency - can be corrected by the use of ergocalciferol 400-2000 IU/day • However in conjunction with other hypocalcemic disorders (e.g., underlying impairments in vitamin D metabolism or renal insufficiency) larger doses may be needed e.g., a 6 to 8 week regimen of 50,000 units, dosed weekly • Severe malnutrition or malabsorption – may require even higher doses
Oral calcium supplements • Calcium carbonate - 40% elemental Ca (Oscal 250 or 500 mg Ca per tablet or Tums ES 400 mg Ca per tablet) • Calcium acetate - 25% elemental Ca (Phoslo) • Calcium Citrate 21% elemental Ca (Citracal) • Dose – 1-2 gm of elemental calcium tid • Should give apart from meals to enhance Ca absorption
Symptoms of severe phosphate depletion (< 1mg/dl) • In general are due to inability to form ATP as well as impaired oxygen delivery due to a decrease in RBC 2,3 DPG: 1) muscle injury - rhabdomyolysis, impaired diaphragmatic function, CHF 2) neurologic - paresthesias, dysarthria, confusion, stupor, seizures, coma 3) hematologic (rare) – hemolysis, thrombocytopenia
Hypophosphatemia treatment • Acute moderate hypophosphatemia (1-2.5 mg/dl) - is common in hospitalized patients, often due to transcellular shifts, if asymptomatic may require no treatment except correction of underlying cause • Acute severe hypophosphatemia (< 1 mg/dl) - may require intravenous P if serious clinical manifestations
Intravenous phosphorus treatment for hypophosphatemia • Total body P deficit – can not be easily determined but has been demonstrated that the dosage listed below can be given safely • Infuse 0.08 to 0.16 mmol/kg in 500 mL of .45% NS over 6 hours and stop when P>1.5 mg/dl (so in a 100 kg patient this is 8-16 mm - order set in Cerner is for 10 mm) • Duration of infusion – it may take 24-48 hours to replenish intracellular stores • Hypocalcemia is the main risk (binding of serum Ca by the P) especially with prolonged infusions; hyperphosphatemia
Phosphorus preparations • Normal dietary P about 1000 mg • 1 mmol P = 31 mg • Neutraphos - 250 mg elemental P, K+ 7 meq, Na+ 7 meq • Neutra-Phos potassium - 250 mg elemental P, K+ 14 meq • Fleets Phospho-Soda – 815 mg P, Na+ 33 meq/ 5 mls • Intravenous K+ phosphate – 1.5 meq KCl/mm PO4 • Intravenous Na+ phosphate - 1.3 meq NaCl/mm PO4 • Intravenous phosphate preparations recently not always available in hospital pharmacies
Hypomagnesemia - signs and symptoms • Nonspecific symptoms – anorexia, nausea, apathy • Hypocalcemia – tetany, seizures, positive Chvostek and Trousseau signs • Hypokalemia – weakness, arrhythmias • Increased susceptibility to ventricular arrhythmias during myocardial ischemia
Significance of low serum Mg in CV disease • Mild hypomagnesemia is common with diuretics • Predisposes to cardiac arrhythmias in the settings of acute ischemic event, CHF, cardiopulmonary bypass, torsades de pointes, or in ICU patients • Myocardial infarction - with low Mg is increased risk of ventricular arrhythmias especially first 24 hours - which risk may be reduced by IV Mg • Torsades de pointes – increased risk with low Mg especially if on class Ia or III antiarrhythmics
Plasma magnesium concentration mg/dL meq/L mmolL Free 1.3 1.1 0.55 Complexed 0.4 0.32 0.16 Protein-bound 0.4 0.32 0.16 Total 2.1 1.76 0.87 (1.9-2.3) (1.5-2.0) (0.7-1.0)
Hypomagnesemia treatment • Severe symptomatic hypomagnesemia (tetany, hypocalcemia, arrhythmias): treat intravenously: e.g., 50 meq IV over 8 to 24 hours, to maintain Mg >1 mg/dl • MgSO4 vial =1 gm MgSO4=96 mg elemental Mg=8 meq • Asymptomatic hypomagnesemia: treat with oral agents
Oral magnesium preparations • Normal daily dietary Mg intake 360 mg • Mag-Ox 400 - 240 mg of elemental Mg per 400 mg tablet • Uro-Mag – 84 mg per 140 mg tablet • Sustained release (Slow-Mag) - 64 mg per tablet • Typically 240 mg of elemental Mg is given for dietary deficiency, more severe deficiency may require up to 720 mg/day elemental Mg • major side effect - diarrhea
Hypermagnesemia • Urinary Mg excretion can increase more than fivefold in response to a Mg load thus hypermagnesemia is typically only seen in the setting of renal failure when a very large Mg load is given intravenous, oral, via enema
Hypermagnesemia - clinical manifestations • Mg 4-6 meq/L – lethargy, drowsiness, diminished reflexes • Mg 6-10 meq/L – somnolence, hypocalcemia, absent reflexes, low BP, bradycardia, EKG changes (with IV Mg in eclampsia usual level 5-7 meq/L) • Mg >10 meq/L – muscle paralysis, complete heart block, cardiac arrest
Hypermagnesemia – signs and symptoms • 3 types of symptoms are seen when Mg >4 meq/L : 1) neuromuscular effects (curare like) 2) cardiovascular effects (Ca and K channel blockade) 3) hypocalcemia (PTH suppression)
Hypermagnesemia – treatment of symptomatic patient • If renal function is normal cessation of Mg allows prompt restoration of normal levels • If renal function is impaired hemodialysis is effective in removing Mg • In cases with severe symptoms 100-200 mg elemental Ca over 5-10 minutes is effective antagonist
Key points • Main risk of IV Mg is giving to azotemia patients and development of hypermagnesemia • Main risk of IV P is binding to serum Ca causing hypocalcemia, usually with prolonged infusions not adequately followed • Main risk of IV Ca - infiltration of vein and tissue necrosis, especially with calcium chloride • If hypocalcemia consider may also be low [Mg] • If hypokalemia consider may also be low [Mg] • Hypermagnesemia – inhibit effects with IV Ca