Download
1 / 69
690 likes | 918 Views
Inflammation AND IMMUNITY Unit II. Overview = Chapter 6: p. 111-119; HIV = Chapter 11: p. 234-258 Anaphylaxis = Chapter 11: p. 263-265 Tuberculosis = Chapter 14: p. 324-329. Infection Prevention and Control. Lesson 6.1 Chapter 6. The Immune System.

E N D
Inflammation AND IMMUNITY Unit II Overview = Chapter 6: p. 111-119; HIV = Chapter 11: p. 234-258 Anaphylaxis = Chapter 11: p. 263-265 Tuberculosis = Chapter 14: p. 324-329
Infection Prevention and Control Lesson 6.1Chapter 6
The Immune System • Immunity: the body’s specific protective response to invading foreign agent or organism • Immunopathology:the study of diseases that result from dysfunction of the immune system • Immune disorders: • Autoimmunity • Hypersensitivity • Immune deficiencies: primary and secondary • Infection
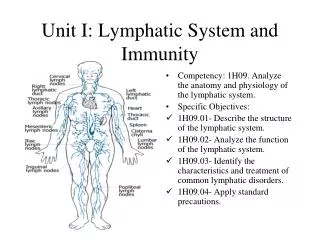
Lymphocytes • B lymphocytes mature in the bone marrow; T lymphocytes mature in the thymus where they also differentiate into cells with various functions
Definitions of Terms Normal flora Vaccines and antimicrobial agents Infection Communicable Disease
Factors Influencing Infection and Disease Intrinsic: Genetic predisposition, age, sex, race, chronic diseases Extrinsic: Personal behaviors (drugs, alcohol, hygiene, sexual practices) and occupation Socioeconomic status (Refer to Table 6-2.)
Disease-Producing Pathogens Airborne, contact, or droplet Bacteria, viruses, protozoa, rickettsiae and chlamydia, fungi, mycoplasmas, and other infectious agents
Primary Lines of Defense The skin The inflammatory response The immune response Normal flora of the host
Mechanical Barriers to Infection Intact skin and mucous membranes Protective covering for the more delicate and vulnerable underlying tissues and organs
Chemical Barriers to Infection Lactic and fatty acids in sweat and the sebaceous glands Lysozyme Stomach acid and digestive enzymes Mucus and cilia
Protective and Defensive Mechanisms Against Infection Innate and acquired immunity (See Box 6-1.) Heredity General health, state of nutrition, hormone balance, immune status, and the presence of a chronic disease
Fever Hypothalamus Increase metabolic and oxygen demand Shivering
Nutrition Young and elderly Excessive stress
Antigen Protein found on the outside of cells “Self” (native) or “non-self” (foreign) Stimulates the immune response to wipe out microorganisms
Antibodies (Immunoglobulins): IgM Appears first if the body is exposed to an antigen Binds to the antigen Works to clear the pathogen from the body
Antibodies (Immunoglobulins): IgG Is the most abundant immunoglobulin Crosses the placental barrier Can be given to provide passive immunity
Antibodies (Immunoglobulins): IgA Is found in tears, mucus, saliva, gastric fluid, colostrum, and sweat Prevents pathogens from attaching to or penetrating epithelial cells, such as the skin
Antibodies (Immunoglobulins): IgE Has the ability to bind to mast cells and basophils When triggered, releases histamine and heparin that in turn stimulate a hypersensitivity reaction Is seen in bronchial asthma or systemic anaphylaxis
Antibodies (Immunoglobulins): IgD Works together with IgM Stimulates certain cells in the immune system Has an unclear overall role in the immune response
Protective and Defensive Mechanisms Against Infection Bone marrow Leukocytosis Phagocytosis Macrophages Liver Normal flora (Refer to Tables 6-3 and 6-4.)
The Inflammatory Response Basic purposes: Neutralize and destroy harmful agents Limit their spread to other tissues in the body by walling off the organisms Prepare the damaged tissues for repair
Inflammatory Changes The cells of the damaged tissues and adjacent connective tissues The blood vessels in and near the site of injury The blood cells, particularly the leukocytes The macrophages and the phagocyte activity The immune system The hormonal system
Signs and Symptoms of Inflammation Local reactions, including redness, swelling, and pain Systemic reactions and common signs/symptoms
Chemical Release and Vascular Changes Complement system Phagocytosis and the inflammatory process Viral infections and interferon Histamine and serotonin Localized swelling or edema
Immune Response The detection of entry by foreign agents as soon as they gain access to the body's cells Immediate recognition of the agents as foreign or alien The ability to distinguish one kind of foreign agent from another and to "remember" that particular agent if it appears again years later
Hormonal Response Cortisone and anti-inflammatory actions Aldosterone as proinflammatory
The Infection Chain Direct or indirect contact Vectors Interaction of agent, host, and mode of transmission Reservoir
Box 6-2: Human Reservoirs Carrier: Person has the actual infection but does not show any obvious signs or symptoms; typically does not take precautions to prevent the spread of infection and can transmit it to others Colonized: Can transmit the pathogenic organisms by either direct or indirect contact with inanimate objects or within her own environment Infectious (symptomatic): Has obvious signs and symptoms of infection; less likely to spread infection as precautions are usually taken
Care of Patients with Immuneand Lymphatic Disorders Lesson 11.1Chapter 11
Stages of HIV Disease • Primary infection • HIV asymptomatic • HIV symptomatic • AIDS
Acquired Immunodeficiency Syndrome Human immunodeficiency virus (HIV) Monogamous relationship Seropositive with HIV Unsafe practices Contact with blood containing HIV through broken skin or mucous membranes (Also see Cultural Cues 11-1.)
Modes of HIV Transmission Unprotected sexual contact Sharing needles with HIV-infected person Occupational exposure Maternal transmission Contaminated blood transfusion Organ transplant from HIV-infected person (Refer to Box 11-1 and Health Promotion Points 11-1.)
Pathophysiology of AIDS HIV is a retrovirus and has reverse transcriptase CD4 lymphocyte HIV-infected people with CD4+ T lymphocyte count >200 cells/mm3 Opportunistic infections (Refer to Figure 11-1 and Table 11-1 for more information.)
Signs and Symptoms of AIDS Sentinel infections Initial flulike symptoms: Fever, fatigue, diarrhea, and loss of appetite Skin rashes, night sweats, swollen lymph glands, and significant weight loss Memory or movement problems Asymptomatic (Refer to Box 11-3 for WHO classification of HIV infection and staging.)
Management of Early HIV Infection Assess eye and mouth condition, neurologic status, skin and lymph nodes, and any signs of opportunistic infection. Perform psychological assessment. Take a sexual and substance use history.
Treatment Non-nucleoside reverse transcriptase inhibitors (NNRTIs) Nucleoside reverse transcriptase inhibitors (NRTIs) Protease inhibitors (PIs) Highly active antiretroviral therapy (HAART) (Refer to Box 11-2 and Table 11-2 for information on HIV tests and medications.)
Complications Opportunistic infections: Viral infections Bacterial infections Fungal infections Parasitic infections (Refer to Table 11-3 for more information.) Neoplasms Neurologic complications
Safety Alert 11-2: Chickenpox Transmission The herpes zoster virus that causes shingles is highly infectious. Any nurse who has not had chickenpox, or been successfully immunized against chickenpox, should not be assigned to care for a patient with herpes zoster. Pregnant nurses should not care for any patient with herpes lesions as the virus may harm the fetus.
Health Promotion Points 11-3: Preventing Toxoplasmosis Toxoplasma gondii, the organism that causes toxoplasmosis, is found in poorly cooked meats, particularly pork, venison, and mutton. It is also found in cat feces. Immunosuppressed or pregnant individuals should not empty cat litter boxes or eat undercooked meat. Children’s sand boxes and dirt play areas are frequently used by outdoor cats as litter boxes. Gardeners routinely come in contact with soil that could be contaminated. Toxoplasma is transmitted by the individual swallowing the organism. Good hand hygiene after contact with contaminated items can help prevent the spread of the organism.
Opportunistic Infections: Viral Infections Herpes simplex types 1 and 2 Herpes zoster (shingles) Cytomegalovirus (CMV) Epstein-Barr virus (EBV) Varicella (chickenpox)
Opportunistic Infections Mycobacteriumtuberculosis (MTb) Mycobacterium avium complex (MAC)
Opportunistic Infections:Fungal and Parasitic Infections Cryptococcosis Histoplasmosis Candida albicans Pneumocystisjiroveci (formerly carinii) pneumonia (PCP) Toxoplasmosis (Toxo) Cryptosporidiosis
Neoplasms and Neurologic Complications Kaposi sarcoma (KS) Non‑Hodgkin's lymphoma (NHL) AIDS dementia or HIV encephalopathy