Download
1 / 18
180 likes | 297 Views
Repeat Trainees: What Are We Learning?. Paul F. Cook, PhD MPAETC Evaluator University of Colorado at Denver & Health Sciences Center. HRSA’s Mission for AETCs. Improve health outcomes of people living with HIV/AIDS through … Training on clinical management of HIV disease in such areas as:

E N D
Repeat Trainees:What Are We Learning? Paul F. Cook, PhD MPAETC Evaluator University of Colorado at Denver & Health Sciences Center
HRSA’s Mission for AETCs • Improve health outcomes of people living with HIV/AIDS through … • Training on clinical management of HIV disease in such areas as: • use of ART and • prevention of HIV transmission • Targeting providers who treat vulnerable populations
Process Number of Trainings (ERs) Number of Trainees (PIFs) Type of Trainees Type of Patients Served by Trainees Impact/Outcome Satisfaction with Training Increased Knowledge Change in Practice Behavior Better Patient Outcomes Types of Evaluation
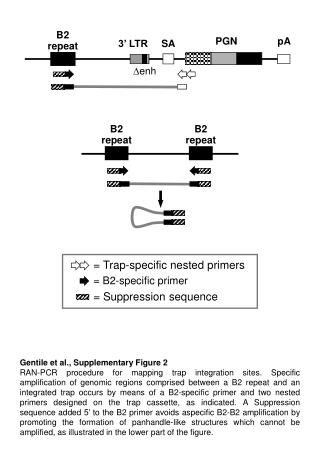
The AETC Data Report (2007) • Across all AETCs, 94,638 trainees filled out a PIF (80%). • There were 60,648 unique individuals (i.e., 36% repeaters) • 88% attended at Levels 1-3 • “More intensive training likely contributes to … impact on clinical practice, however, … documentation of such outcomes is … beyond the scope of this [report].” (p.9)
Studying Repeat TraineesAims of the Current Study #1 – Determine whether AETC trainees change their practice behavior over time #2 – Test the relationships between satisfaction, knowledge gain, intent to change, and actual practice behavior change #3 – Evaluate level of training as a predictor of outcome
Participants • FY2006-2007, first 3 quarters • MPAETC trainees (one LPS not included – data problems) • Attended 2+ events each • Completed a PIF (with a valid PIF ID) and “Quality of Presentation” (QOP) evaluation form each time • N = 402 PIFs;1,395 attendees; or about 10% of unique IDs
Population 70% Female Discipline: 22% MD/PA 9% Pharm 10% Dental 28% MH/Other 87% White 4% AI/AN 38% clinicians 19% see HIV+ pts (M = 29) Sample 74% Female Discipline: 33% MD/PA 16% Pharm 2% Dental 19% MH/Other 83% White ½% AI/AN 41% clinicians 38% see HIV+ pts (M = 55) Sample Representativeness
Procedure • All MPAETC sites use QOP • Levels 1-2: QOP form at end of each training event, linked via PIF ID • Level 3: QOP items pretest/ posttest, same PIF ID • All data stored in central Access database • Query to identify repeaters • Data analysis using HLM 6.0
Instrument – QOP-2 • 2006 adaptation of existing tool by Vojir et al. • Subsections measure: • Trainee satisfaction (5 items) • Intent to change (1 item) • Pretraining knowledge (1 item, retrospective) • Posttraining knowledge (1 item) • Practices w/ HIV- pts (3 items) • Practices w/ HIV+ pts (4 items)
Instrument Psychometrics • Satisfaction: alpha = .77; • Knowledge: retest reliability (eta2) = .97; subjective change correlates r = .32 with improvement on a test • Practice Behavior items: retest reliability (r) = .76-.95; subscale alphas = .91-.94 • Weak or moderate correlations across domains
Analysis Plan • Hierarchical Linear Modeling to determine change within participants • Key predictor = time • Initial coding: days since first event for that participant • Final coding: event number (starting from 1) for that participant, since 7/1/06
1. Training → Behavior Change • T = 2.41, p = .016 • Small r = .09 • Significant for number of trainings, not for days • Effect on total & HIV+; not HIV-
Bonus Finding: CDC Testing • Recommendations released 9/22/06 on universal testing • HLM for repeat trainees • total Bx, T = 2.77, p = .006 • No effect on testing, but risk assessment, prevention! • No effect on any other behavior variable • Caveat: only for repeaters
2. Other Outcomes • Time → Δ Satisfaction, Knowledge or Intent • Satisfaction → Δ Knowledge & Δ Intent • Higher Pretest Knowledge → • Posttest Knowledge, but • Δ Knowledge and Intent • Δ Knowledge → Δ Intent • Satisfaction, Intent, Knowledge → Δ Behavior
3. Effect of Training Level • Whether a participant attended a Level 3 event had no effect on behavior • Percent of all trainings attended that were Level 2 did have a significant effect: T = 2.79, p = .006 • Some support for the idea that higher training levels produce better outcomes
What Changes HCP Behavior? • Number of trainings led to behavior change • Mainly for HIV+ patient care • More level 2 events led to behavior change • Mainly for HIV- patient care • CDC recommendations led to behavior change • Mainly for risk assessment and prevention
Limitations/Future Directions • Longer follow-up needed • Higher % repeaters possible • Greater change possible • Results need replication • Repeaters may be unusual • Diverse groups, esp. AI/AN • More non-“HIV providers” • Measure may show ceiling effects for expert trainees • Pilot separate “expert” items
Thank You If we knew what we were doing, it wouldn’t be called ‘research.’ —Albert Einstein