Download
1 / 27
320 likes | 394 Views
Psoriatic arthritis. Department of Rheumatology and Connective Tissue Diseases Tacjana Barczyńska. Psoriatic arthritis (arthritis psoriatica, psoriatic arthritis, PsA). a chronic inflammatory disease different phenotypes seronegative spondyloarthropathy

E N D
Psoriatic arthritis Department of Rheumatology and Connective Tissue Diseases Tacjana Barczyńska
Psoriatic arthritis(arthritis psoriatica, psoriatic arthritis, PsA) • a chronic inflammatory disease • different phenotypes • seronegative spondyloarthropathy • most often develops in patients with psoriasis The order of developing: • arthritis or enthesitis • changes in skin and nails may vary, but usually psoriasis develops earlier than arthritis The severity of psoriasis typically does not correlate with the degree of joint damage.
PsA- epidemiology • PsA affects0,05-0,24% of the Caucasian population • Psoriasis affects2-3% of the popluation • PsA affects6-42%(~40%) of patients with psoriasis Women: Men– 1 :1 (equal sex prevalence) • W- symmetrical polyarthritis • M- type with predominant symptoms of spondyloarthropathy (axial) The onset of symptoms • usually between 20-50 years old • may also occur in children
Ethiopathogenesis- genetic factors Epidemiological data: • 40% of patients with PsA have first-degree relatives diagnosed with psoriasis or PsA • PsA more often develops in monozygotic twins • PsA identified in both parents-greater risk of developing PsA Antigens in PsA: • HLA-B27 (axial form) • HLA-Cw6 (predisposes to skin psoriasis and correlates with the development of psoriasis at a younger age)
Ethiopathogenesis- immunological mechanisms • Activation and expansion of keratinocytesand synoviocytes • Infiltration by mononuclear cells and angiogenesis • Increased immune, humoral and cellularresponse • increased proinflammatorycytokine expression, especially TNF in skin and joint fluid
Ethiopathogenesis- environmental factors • mechanical injury • bacterial infections (e.g. streptococci) • viral infections (e.g. HIV infection- 10x higher risk of developing PsA)
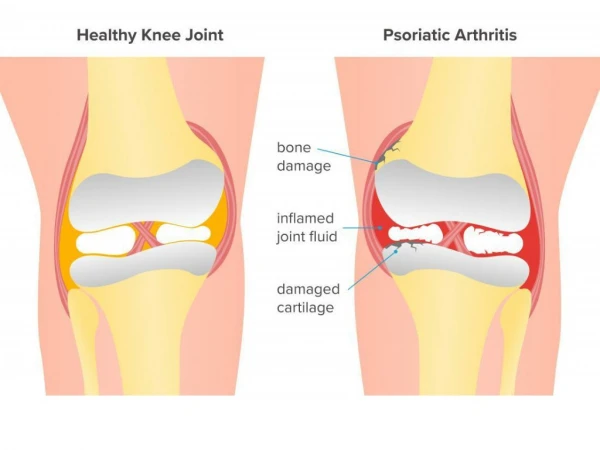
Ethiopathogenesis Active inflammation in PsA leads to bone remodeling- coexistence of two mechanisms: • resorption- damage to the articular cartilage and bone • creation of new pathological bone structures (e.g. ankylosis)
Classification of PsA PsA classification proposed by Moll and Wright is helpful in the diagnosis of early forms of PsA. However, over time the characteristics of the various types can overlap. Some authors prefer PsA division into 3 types: • peripheral arthritis • peripheral arthritis with involvement of the spine • type with predominant symptoms of spondyloarthropathy (axial)
Clinical presentation of PsAPeripheral arthritis • inflammation of one or more joints • recurrent exudative arthritis of the lower limbs (eg. knee) • symptoms of inflammation (pain, swelling, redness, increased warming and stiffness of the affected joint) • asymmetric joints involvment, especially in the early stages of the disease • when the process involves increasing number of joints- changes may be symmetical
Peripheral arthritis Polyarticular symmetrical form can resemble RA, differentiating elements: • absence of rheumatoid factor and rheumatoid nodules • joint involvement: DIP • changes in the nail plate Arthritis mutilans- severe deformities • Telescopic fingers • Subluxation
Clinical presentation of PsAThe axial form Involvement of joints of the spine and sacroiliac joints: • changes are usually one-sided (unilateral) • inflammatory spinal pain (back pains) • limitation of motion of the spine
Fingers inflammation (dactylitis)- • may be the first symptom of PsA • occurs in 40-48% cases of PsA • Dactylitis of toes or fingers (65%only toes) • inflammatory process involves primarily the tendon and tendon sheath of the flexor, and then the remaining structures- PIP and DIP joints, bones and soft tissues, leading to joint destruction Types of dactylitis: • acute- swelling, redness and pain around the toe or finger • chronic- despite the resolution of active inflammation persists painless swelling of the whole toe or finger
Enthesitis Inflammation of the ligament, tendon or joint capsule at the site of attachment to the bones, revealed pain and swelling. Location of changes in PsA: • most often- inflammation of the Achilles tendon and plantar fascia • rarely- tendons in the knee, shoulder, elbow
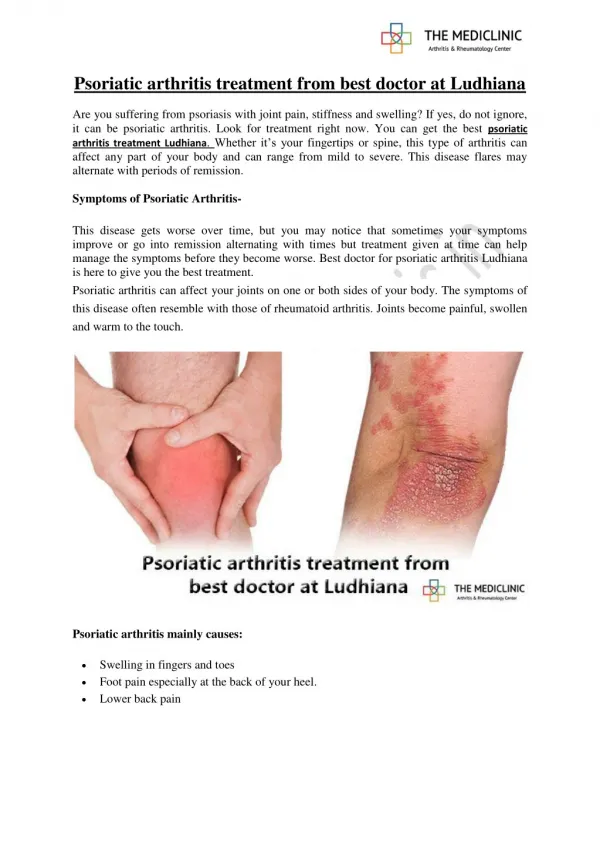
Psoriasis • 70%- psoriasis precedes the appearance of arthritis • 15%-simultaneous occurrence of skin lesions and arthritis • 15%- arthritis is the first symptom of the disease, and psoriasis may develop after a few years (psoriatic arthritis sine psoriasis) Primary eruption- red-brown lump of clear boundaries with silvery scales Psoriasis - location: • knees, elbows, umbilicus, scalp, natal cleft, external genitalia, but also the trunk, hands and feet
Nail psoriasis • 80% patients with PsA • 20-40% patients with psoriasis and unchanged joint • may be a predictor of PsA, particularly the form with DIP joint involvement • may be the only clinical manifestation of the disease Psoriatic nail changes: • Nail pits- point depressions in the nail plate • longitudinal or transverse grooves • yellow and white discoloration • ,, oil spots” • onycholysis- separation of the nail from its bed
Ocular Symptoms • conjunctivitis • uveits Uveitis • symptoms: pain, redness, blurred vision • can lead to blindness
The diagnosis of PsA • Personal and family history of psoriasis • Physical examination: evaluation of skin lesions, nail, peripheral joints, sacroiliac, spine, tendon and fingers • Basic laboratory tests, including ESR and CRP • Rheumatoid Factor • Imaging studies of joints and tendon (X-ray, ultrasound, MRI) • Genetic testing: HLA-B27 and HLA-Cw6 • Dermatological consultation
CASPARClASsification criteria for Psoriatic ARthritis(sensitivity 91.4%, specificity 98.7%)
X-rays of hands and feet • changes present in the DIP joints • asymmetry • rarely periarticular osteopenia • simultaneously destructive lesions (erosions, geodes inflammatory osteolysis) and proliferation of bone (periosteal new bone, often juxta-articular) • osteolytic lesions within the phalanges of the nail provide a picture of the so-called sharpened pencil, and when accompanied by a proliferation of bone tissue damaged joint is similar to ,,pencil in the cup "
PsA- axial form Atypical syndesmofites Sacroiliitis
Differential diagnosis • RA • osteoarthritis • gout • Infectious arthritis • Other inflammatory spondyloarthropathies (ankylosing spondylitis, reactive arthritis and arthritis in the course of inflammatory bowel diseases)
The active form of PsA: presence of ≥1 tender joint and / or enthesitis and / or inflammation of the finger (dactylitis) and / or inflammatory back pain. • Poor prognosis factors: inflammation of the joints ≥5, elevated acute phase markers (ESR and CRP), progressive damage in X-ray, previous use of GKS, loss of function and reduced quality of life.
Synthetic DMARDs • Should be used in patients with active peripheral arthritis and factors of poor prognosis. • Early application - several weeks to a maximum of one year. • The drug of first choice is methotrexate (at an optimum dose of 25 mg / week). • No synthetic DMARDs demonstrated efficacy in treating tendonitis and axial disease. • Other DMARDs: sulfasalazine, leflunomide and cyclosporine A
Glucocorticoids • GKS applied topically can be used for enthesitis and dactylitis. • GKS can be used systemically in the lowest possible doses with caution as the relative potential for exacerbation of skin lesions.
TNF-α inhibitors • If despite of the use of synthetic DMARDs within 3-6 months remission or low disease activity is not achieved, consider the inclusion of TNF-α inhibitor in combination with synthetic DMARDs or alone.
Axial form of PsA • The drug of first choice should be NSAIDs. • In the case of high disease activity (BASDAI ≥ 4) TNF-α inhibitor can be considered, even without prior treatment with synthetic DMARDs.