Download
1 / 24
430 likes | 1.03k Views
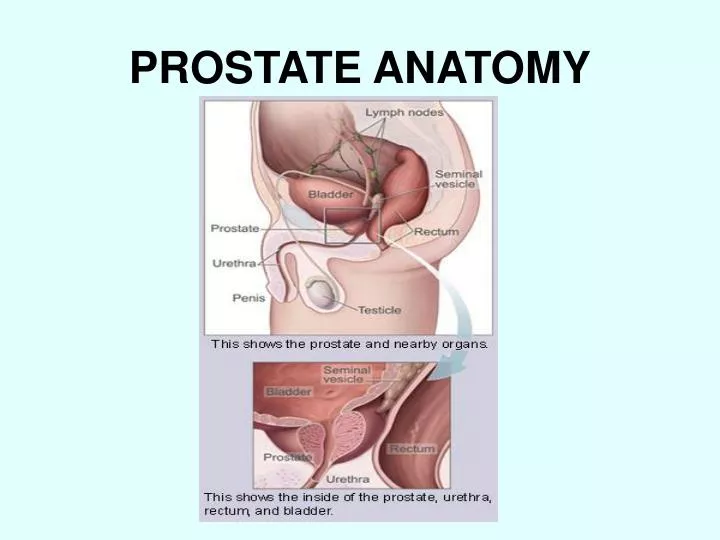
PROSTATE ANATOMY. PROSTATE CANCER STATISTICS Number 1 cancer in men 192,280 new cases estimated for 2009 with 27,360 Deaths 300,000 by year 2015 2010 cases in Mississippi in 2008 with 290 deaths. WHY DO I NEED A DIGITAL RECTAL EXAM AND PSA ?. MALE CANCER RATES. % Cancers.

E N D
PROSTATE CANCER STATISTICS Number 1 cancer in men 192,280 new cases estimated for 2009 with 27,360 Deaths 300,000 by year 2015 2010 cases in Mississippi in 2008 with 290 deaths WHY DO I NEED A DIGITAL RECTAL EXAM AND PSA ?
MALE CANCER RATES % Cancers
RISK OF PROSTATE CANCER BY AGE* • < 39 years 1 in 10,100 • 40-59 years 1 in 38 • 60-79 years 1 in 14 • Lifetime 1 in 6 *American Cancer Society 2006
TUMOR STAGING • STAGING DESCRIBES THE EXTENT OR SEVERITY OF A TUMOR • Staging helps the doctor plan a person’s treatment. • The stage can be used to estimate the person’s prognosis (likely outcome or course of the disease).
T STAGE (EXTENT OF THE TUMOR) • TX: Primary tumor cannot be assessed • T0: No evidence of primary tumor • T1: Clinically unapparent tumor not palpable nor visible by imaging • T1a: Tumor incidental histologic finding in 5% or less of tissue resected • T1b: Tumor incidental histologic finding in more than 5% of tissue resected • T1c: Tumor identified by needle biopsy (e.g., because of elevated PSA) • T2: Tumor confined within prostate* • T2a: Tumor involves 50% or less of one lobe • T2b: Tumor involves more than 50% of one lobe but not both lobes • T2c: Tumor involves both lobes • T3: Tumor extends through the prostate capsule** • T3a: Extra capsular extension (unilateral or bilateral) • T3b: Tumor invades seminal vesicle(s) • T4: Tumor is fixed or invades adjacent structures other than seminal vesicles: bladder neck, external sphincter, rectum, levator muscles, and/or pelvic wall
PROGNOSTIC FACTORS • STAGE • GLEASON’S SCORE • PSA LEVEL • PERCENT OF POSITIVE BIOPSIES • PATIENT AGE AND HEALTH
TREATMENT OPTIONS • RADICAL PROSTATECTOMY • EXTERNAL BEAM RADIATION • BRACHYTHERAPY • CRYOTHERAPY • WATCHFUL OBSERVATION
WHAT IS BRACHYTHERAPY? • BRACHYTHERAPY IS A FORM OF RADIOTHERAPY WHERE A RADIOACTIVE SOURCE IS PLACED INSIDE OR NEXT TO THE AREA BEING TREATED. • BRACHYTHERAPY IS COMMONLY USED TO TREAT LOCALIZED PROSTATE CANCER.
Prostate cancer is well suited to brachytherapy. The prostate gland is located under the bladder and in front of the rectum. The gland is encapsulated allowing the radiation to be focused in the prostate to avoid serious side effects. The prostate gland is also close enough to the skin that it can be easily accessed by brachytherapy needles.
Brachytherapy involves injecting radioactive seeds into the prostate gland. They give off their radiation at a low dose rate over several months. The seeds remain in the prostate gland permanently.
PROSTATE BRACHYTHERAPY IS PERFORMED AS A TWO STAGE PROCEDURE • STAGE 1- THE VOLUME STUDY • STAGE 2- THE SEEDS IMPLANT
VOLUME STUDY • Ultrasound images of the prostate are obtained every 5 mm with a transrectal ultrasound probe. Done as an outpatient procedures, this takes about 30 minutes. During the volume study a catheter is placed in the bladder to identify the water pipe (urethra). • The images are downloaded into the treatment planning computer to create a three dimensional model of the prostate that will be used to plan the seed placement. • This plan will be unique to each patient and will determine the position and number of seeds needed. • The seeds are then ordered for each individual patient.
SEEDS IMPLANTATION • The implant is done under general anesthesia in OR. • Radioactive seeds are implanted into the prostate gland under transrectal ultrasound guidance, using needles that pass through the skin between the legs behind the scrotum (the perineum). • Each needle may deliver between 2-6 seeds and, usually, 20-30 needles are required to implant 80-140 seeds. • The seeds are woven into a strand of absorbable material to help maintain their position and reduce the risk of seed migration. • The procedure takes about 90 minutes and after recovery the patient can go home.
EXTERNAL BEAM RADIATION • At the Forrest General Cancer Center we use state of the art Varian linear accelerators coupled with IMRT and IGRT technology to deliver accurate focused beams to destroy the cancer cells within the prostate gland.
INTENSITY MODULATED RADIATION THERAPY • IMRT, is a state-of-the-art radiation delivery system offered at the Forrest General Cancer Center. • It has been called the most significant breakthrough in radiation treatments in the past 30 years. • IMRT can treat difficult-to-reach tumors with new levels of accuracy such as tumors in the spine, head, neck, prostate, lung, liver, and brain. • We are able to use higher radiation doses than traditional methods would allow in these areas, and yet spare more of the surrounding healthy tissue, compared to standard radiation therapy. • During IMRT, small beams (beamlets) with varying intensities of radiation are aimed at a tumor from many angles. • The intensity of each beamlet is tightly controlled, allowing the radiation oncologist to deliver higher doses of radiation to the tumor while significantly reducing the chances of damaging surrounding healthy tissue.
WHAT IS IGRT? • Image-guided radiation therapy is conformal radiation treatment guided by imaging equipment, such as a CT scan, taken in the treatment room just before the patient is given the radiation treatment. • IGRT allows radiation to be delivered to tumors with more precision and allows the physician to account for any organ movement since the last treatment.
WHY IS ORGAN MOTION IMPORTANT DURING EXTERNAL BEAM RADIATION THERAPY? • Organ motion causes physicians to virtually attempt to treat a moving target with a fixed radiation beam. • Because prostate organ motion during the delivery of radiation therapy is unpredictable and variable, ineffective delivery of radiation treatment to the prostate and damage to surrounding healthy tissue may occur.
FIDUCIAL MARKERS The use of fiducial markers for prostate cancer and portal imaging integrated with linear accelerators provide high quality images which can now be used for 3D verification of the actual daily target position.