Download

1 / 35
410 likes | 767 Views
Malnutrition. Protein / Energy. Definitions of Malnutrition. Kwashiorkor: protein deficiency Marasmus: energy deficiency Marasmic/ Kwashiorkor: combination of chronic energy deficiency and chronic or acute protein deficiency Failure to thrive: marasmus in U. S. children under 3.

E N D
Malnutrition Protein / Energy
Definitions of Malnutrition • Kwashiorkor: protein deficiency • Marasmus: energy deficiency • Marasmic/ Kwashiorkor: combination of chronic energy deficiency and chronic or acute protein deficiency • Failure to thrive: marasmus in U. S. children under 3.
Definitions of Malnutrition PEM • Primary: inadequate food intake • Secondary: result of disease FTT • In-organic: inadequate food intake • Organic: result of disease
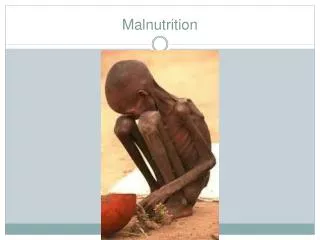
MARASMUS • Marasmus is the term used for severe PEM and wasting (low wt/ht). • Many secondary forms of marasmic PEM are associatedw ith chronic diseases( cysricf ibrosis, tuberculosis,cancer, acquired immunodeficiency virus, celiac disease). • The principal clinical manifestarion in a child wirh severe malnutririon is emaciation with a body weight less than 50%o f the median (50th percentile) for age or less than70%o f the ideal weight For height and depleted body fat stores
Loss of muscle mass and subcutaneous fat stores are confirmed by inspection or palpation and quantified by anthropometric measurements. • the head may appearlarge but generally is proportional to the body length. • Edema usually is absent. • The skin is dry and thin, and the hair may be thin, sparse, and easily pulled out. • Marasmic children may be apathetic and weak
Bradycardia and hypothermia signify severe and lifethreatening malnutririon. • Atrophy of the filiform papillae of the tongue is common) and monilial stomatitis is frequent. • Inappropriate or inadequate weaning practices and chronic diarrhea are common findings in developing countries. • Stunting (impaired linear growth (Table 30-1) results from a combination of malnutrition, especially micronutrients, and recurrent infections. • Stunting is more prevalent than wasting
KOWASHIORKOR • Kwashiorkor is hypoalbuminemic, edematous malnutrition and presents with pitting edema that srarts in the lower extremities and ascends with increasing severity. • It is classically described as being caused by inadequate protein intake in the presence of fat to good caloric intake. • Other factors, such as acute infection, toxins, and possibly specific micronutrient or aminoacid imbalances,are likely to contribute to the etiology
The major clinical manifestation of kwashiorkor is that the body weight of the child ranges from 60%to 80% of the expected weight for age • weight alone may not accurately reflect the nutritional status because of edema
Physical examination reveals a relative maintenance of subcutaneous adiposetissue and a marked atrophy of muscle mass. • Edema varies from a minor pitting of the dorsum of the foot to generalized edema with involvement of the eyelids andscrotum. • The hair is sparse; is easily plucked; and appears dull brown, red, or yellow-white. • Nutritional repletion restores hair color, leaving a band of hair with altered pigmentation followed by a band with normal pigmentation(flag sign)
Skin changes are common and range from hyperpigmentedhyperkeratosis to an erythematous macular rash (pellagroid) on the trunk and extremities. • In the most severe form of kwashiorkor, a superficial desquamation occurs over pressure surfaces ("flaky paint" rash). • Angular cheilosis, atrophy of the filiform papillae of the tongue, and monilial stomatitis are common. • Enlarged parotid glands and facial edema result in moon apathy and disinterest in eating are typical of kwashiorkor.
Examination of the abdomen may reveal an enlarged, soft liver with an indefinite edge. • Lymphatic tissue commonly is atrophic. • Chest examination may reveal basilar rales. • The abdomen is distended, and bowel sounds tend to be hypoactive
History • Marasmus well known for centuries • Kwashiorkor: Cicely Williams • Ga tribe in Ghana “the sickness the older child gets when the next baby is born” • Starch edema, sugar babies • Similar but different diseases
How many? • 36% of children in the world are underweight • 43% stunted • 9% wasted • Better nutrition, but more children in high risk areas, yields more children affected.
Causes • Social and Economic • Poverty • Ignorance • Inadequate weaning practices • Child abuse • Cultural and social practices • Vegan • Low fat diets
Biologic factors • Maternal malnutrition, prematurity • Start life with poor stores • Infectious disease • Diarrhea, Aids, TB, measles • Environmental • Unsanitary living, poor quality water • Agricultural/cultural patterns • Droughts, floods, wars, forced migrations
Age of child • Infants and young children • High nutritional needs • Early weaning or late weaning • Poor hygiene • Marasmus < 1 year • Kwashiorkor >18 months with starchy weaning foods
Pathophysiology • Develops slowly, adapts to decreased intake • Marasmus • Less fragile metabolic equilibrium • Less effective adaption or acute problem • Kwashiorkor, mixed
Energy • Decreased intake yields decreased activity • Decreased play and physical activity • Mobilization of body fat, weight loss, • Subcutaneous fat • Muscle wasting • Maintains visceral protein in marasmus • Nl albumin • Larger protein deficit leads to faster visceral protein falls and edema.
Marasmus Weight loss Nl or low protein Boarderline hgb, hct NL AA profile Nl blood glucose Nl enzymes Nl transaminase Kwashiorkor NO weight loss High extracellular water Low hgb, hct Low protein Elevated AA profile Low enzymes High transaminase Biologic differences
Pathophysiology • Cardiac • Output, heart rate and blood pressure decrease • Postural hypotension • Immune system • T lymphocytes and complement decreased • Susceptible to bacterial infection • Cytokines (glycoproteins) • Poor immune response • TNF inc leading to anorexia, muscle wasting and lipid changes
Pathophysiology • Decreased total body potassium • Not electrolytes, but problem in rehabilitation • GI function • Poor absorption of lipids, and sugars • Decreased enzyme and bile production • Increase incidence of diarrhea, and bacterial overgrowth
Pathophysiology CNS • Decreased brain growth and myelnation • Electrical changes similar to dylexia Parental adaptation • Increased breastfeeding • Altered expectations
Diagnosis • Anthropometry • Acute: Wasting: low weight for height • Chronic: Stunted: low height for age • 4 groups • Normal • Wasted not stunted: acute PEM • Wasted and stunted: acute and chronic PEM • Stunted not wasted: past PEM, nutritional dwarfs
Diagnosis • Normal: ± 1 SD • Mild: -1.1 to -2 SD • Moderate -2.1 to -3 SD • Severe greater than -3 • Less than 5th percentile in US • BMI in adolescents • Moderate <15 ages 11-13, <16.5 ages 14-17 • Severe <13 ages 11-13, <14.5 ages 14-17
Diagnosis • Mild to moderate • Weight loss if acute, decreased growth velocity of chronic • Decreased activity • Marasmus • Skin and bones, thin hair, monkey face • Hypoglycemia, hypothermia
Diagnosis • Kwashiorkor • Soft pitting edema, starting in feet and legs • Skin lesions • Skin dry, with hyperkeratosis and hyperpigmentation • Preserved fat layer, small weight deficit, ht may be normal • Dry brittle hair • Anorexia, with vomiting and diarrhea
Diagnosis • Mixed • Edema, with or without skin lesions • Muscle wasting and loss of subcutaneous fat
Treatment • Acute/ life threatening • Fluid and electrolyte • K and Mg shifts • Oral rehydration, slowly 70-100 ml/kg • Infections: main cause of death • Aggressive treatment, but disease alters metabolism of drugs • Other deficiencies • Anemia and heart failure, care with transfusions and no diurretics • Vitamin A: immediate treatment
Treatment • Slow re-feeding • Small frequent feeding around the clock • Patient encouragement of food • Nutritional rehabilitation • Play and teaching • controlinfections
Recovery? • At home • Reach weight for height and replete muscle mass • Normal is 25-75% weight for height and continue for one months after • Treat other deficiencies • Family problems • Who does this include here? • Tube feeding. • Disabilities • FTT
What does it mean? • Poverty • Correlation of income, wt, ht and hgb in US • What is wealth? • Importance of food choice • Brain development • Iron deficiency: neuro transmitters • Brain waves:
What does it mean? • Learning: • Difference in treatment by parents • Duration of breastfeeding • Expectations • Long term effects • INCAP two villages, one protein and one calorie • At 18 protein supplemented group had higher performance scores irrespective of educational exposure. They had taught themselves.
What does it mean? • Learning: • Difference in treatment by parents • Duration of breastfeeding • Expectations • Slums of Kingston, Jamaica • Educational intervention, early rise plateau • Nutritional intervention, late rise • Additive effect • Education lasts, not nutrition, but high IQ mom’s and nutrition group did as well as education.
Implications • Children learn by interacting with the environment • Poverty: limited environment • Malnutrition: limited interaction • Additive effect! • Loss to society of human potential • Lead graph