Download
1 / 18
590 likes | 1.47k Views
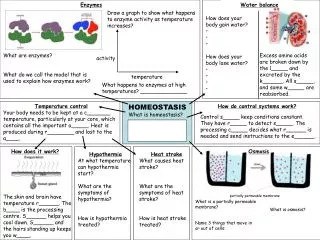
Water Homeostasis . • The body maintains a balance of water intake and output by a series of negative feedback loops involving the endocrine system and autonomic nervous system. .

E N D
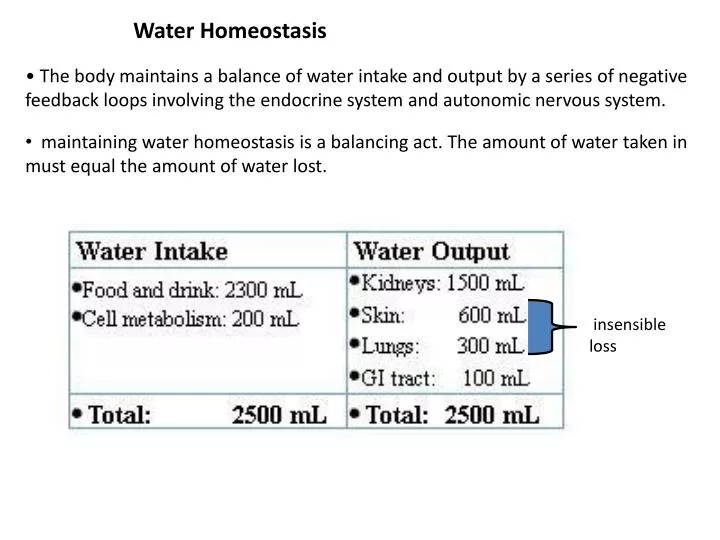
Water Homeostasis • The body maintains a balance of water intake and output by a series of negative feedback loops involving the endocrine system and autonomic nervous system. • maintaining water homeostasis is a balancing act. The amount of water taken in must equal the amount of water lost. insensible loss
Disturbances of Water Homeostasis Hypervolemia • Hypervolemia occurs when too much water and solute are taken in at the same time. Although extracellular fluid volume increases, plasma osmolarity may remain normal. Overhydration • Overhydration occurs when too much water is taken in without solute. Volume increases, but because solute is not present, plasma osmolarity decreases. Hypovolemia • Hypovolemia occurs when water and solutes are lost at the same time. This condition primarily involves a loss of plasma volume. Plasma osmolarity usually remains normal even though volume is low. Dehydration • When water, but not solute, is lost, dehydration occurs. • Dehydration involves a loss of volume but, because solutes are not lost in the same proportion, plasma osmolarity increases. i.v., infussion of isotonic solution Drinking too much water Blood loss sweating
Mechanisms of Fluid Balance • Four primary mechanisms regulate fluid homeostasis: 1)Antidiuretic hormone or ADH 2)Thirst mechanism 3)Aldosterone 4)Sympathetic nervous system • Thirst Mechanism • • The thirst mechanism is the primary regulator of water intake and involves hormonal and neural input as well as voluntary behaviors. • • Stimulation of the thirst center in the hypothalamus gives you the desire to drink. • • There are three major reasons why dehydration leads to thirst: • 1. When saliva production decreases, the mouth and throat become dry. Impulses go from the dry mouth and throat to the thirst center in the hypothalamus, stimulating that area. • 2. When you are dehydrated, blood osmotic pressure increases, stimulating osmoreceptors in the hypothalamus and the thirst center in the hypothalamus is now further activated. • 3. Decreased blood volume causes a decrease in blood pressure that is signaled by baroreceptors and stimulates the release of renin from the kidney. This causes the production of angiotensin II which stimulates the thirst center in the hypothalamus.
Sympathetic Stimulation in the Nephron • Release of neurotransmitters from the sympathetic nerves in the kidney stimulates smooth muscle cells in the afferent arteriole to constrict. • This process causes a decrease in blood flow into the glomerulus and a drop in glomerular filtration rate and results in less urine formation. Less water leaves the body. • Sympathetic stimulation also causes the release of reninwhich, by stimulating aldosterone secretion, will increase the reabsorption of sodium. • As a result, blood volume will stop decreasing and blood pressure may stabilize. However because the blood pressure and blood volume have not yet returned to normal, the baroreceptors will continue to be stimulated to prevent further loss of blood volume. • In order to bring this person back into to homeostasis, we need to increase the blood volume by drinking fluids.
FREE-WATER CLEARANCE Free water is defined as distilled water that is free of solutes (or solute-free water). In the nephron, free water is generated in the diluting segments, where solute is reabsorbed without water. The diluting segments of the nephron are the water-impermeable segments: the thick ascending limb and the early distal tubule. Measurement of free-water clearance (CH2O) provides a method for assessing the ability of the kidneys to dilute or concentrate the urine. The principles underlying this measurement are as follows: When ADH levels are low, all of the free water generated in the thick ascending limb and early distal tubule is excreted (since it cannot be reabsorbed by the collecting ducts). The urine is hyposmotic, and free-water clearance is positive. When ADH levels are high, all of the free water generated in the thick ascending limb and the early distal tubule is reabsorbed by the late distal tubule and collecting duct. The urine is hyperosmotic, and free-water clearance is negative.
Measurement of CH2O calculated by the following equation: CH2O can be zero, it can be positive, or it can be negative. CH2O is Zero– Isosthenuria where CH2O Free-water clearance (mL/min) V Urine flow rate (mL/min) Cosm Clearance of osmoles (mL/min) [U]osm Urine osmolarity (mOsm/L) [P]osm Plasma osmolarity (mOsm/L) CH2O is positive- Diabetes Insipidus. CH2O is negative- SIADH
Electrolyte Homeostasis • The fluid surrounding the cells in the body must maintain a specific concentration of electrolytes for the cells to function properly. • Electrolytes are a major component of body fluids. They enter the body in the food we eat and the beverages we drink. • While electrolytes leave the body mainly through the kidneys by way of the urine, they also leave through the skin and feces. • Severe vomiting and diarrhea can cause a loss of both water and electrolytes from the body, resulting in both water and electrolyte imbalances. • The concentrations of electrolytes in body fluids must be maintained within specific limits, and even a small deviation outside these limits can have serious or life-threatening consequences. • In this topic we will concentrate on the three most clinically significant electrolytes sodium ions, potassium ions, and calcium ions.
Sodium Homeostasis • The normal concentration range of sodium in the plasma is 136 - 145 milliequivalents per liter, making sodium the ion with the most significant osmotic effect in the extracellular fluid. 145 136 • Hypernatremia • • what will happen if the sodium concentration of the blood plasma increases, as in hypernatremia. • • What effect would this increase in sodium concentration have on the cells that are bathed by the interstitial fluid? • ___ Cells swell • ___ Cells shrink • • The high concentration of sodium in the extracellular fluid exerts osmotic pressure and helps determine the fluid levels in the intracellular space. • Hyponatremia • • What effect would this decrease in sodium concentration have on the cells that are bathed by the interstitial fluid? • ___ Cells swell • ___ Cells shrink • • The water moves into the cell, and the cell expands slightly.
Roles of Sodium in the Body • • nerve impulse conduction and muscle contraction, • primary regulator of water movement in the body because water follows sodium by osmosis. • • If sodium levels in the plasma change, those changes determine fluid levels in the other compartments. Causes and Symptoms of Hypernatremia Which of these reasons would most likely cause hypernatremia in the marathon runner? ____ Too much sodium added ____ Too much water lost Symptoms of hypernatremia include non-specific signs of central nervous system dysfunction such as confusion and lethargy, and in severe cases, seizures and death. • What do you think causes these symptoms? ___ Neurons shrink ___ Neurons swell What will happen to urine output? Decreases • When plasma osmolarity increases, antidiuretic hormone is released, resulting in reabsorption of water and decreased urine output.
Where Does Na+ Reabsorption Occur? FE = 10% [Na+]=145 FE = 3% FE = 35% FE = 0.1 - 2% [Na+] units = mmole/L FE= Fractional excretion
The Na+/K+-ATPase Drives Na+ Reabsorption All Along The Renal Tubule Lumen Blood Na+ 3Na+ ATP ADP 2K+ diuretics Na+
In Early Proximal Tubule Na+ Absorption Is Linked To Nutrient Transport….. Lumen Blood 3Na+ Na+ ATP ADP 2K+ nutrient Nutrient (a.a & gluc.) Familial renal glycosuria – SGLT2 mutations Cystinuria – dibasic amino acid carrier Hartnup’s disease – neutral amino acids
Absorption Mechanisms Change Along The Proximal Tubule inulin 2.0 1.5 Cl- [TFx/Px] Na+ 1.0 osm HCO3- 0.5 Glucose/amino acids 0.0 Length of proximal tubule
Na+ Uptake In The TALH Is Via A Cotransport Mechanism Blood Lumen 3Na+ Na+ NKCC2 2Cl- 2K+ K+ Cl- ROMK CLC-Kb + cations Na, Ca and Mg Mutations in any of NKCC2, ROMK or CLC-Kb = BARTTER’S SYNDROME ADH targets NKCC2 & ROMK ‘loop diuretics’ Bumetanide & Furosemide block NKCC2
Early Distal Tubule Uses Na/Cl Cotransport For Na+ Absorption Lumen Blood 3Na+ Na+ NCCT 2K+ Cl- Cl- NCCT mutations cause GITTELMAN’S SYNDROME Thiazide Diuretics block NCCT
Na+ Entry In The Collecting Duct Is Via An Ion Channel Lumen Blood Principal cell Na+ ENaC 3Na+ K+ ROMK 2K+ ENaC gain of function = LIDDLE’S SYNDROME ENaC loss of function = PSEUDOHYPOALDOSTERONISM (PHA) Aldosterone activates ENaC & ROMK while Amiloride like diuretics block ENaC