Download
1 / 57
950 likes | 1.36k Views
NASO-GASTRIC FEEDING TUBE INSERTION. Prepared by: Imran Iqbal Clinical Instructor. DEFINITION.

E N D
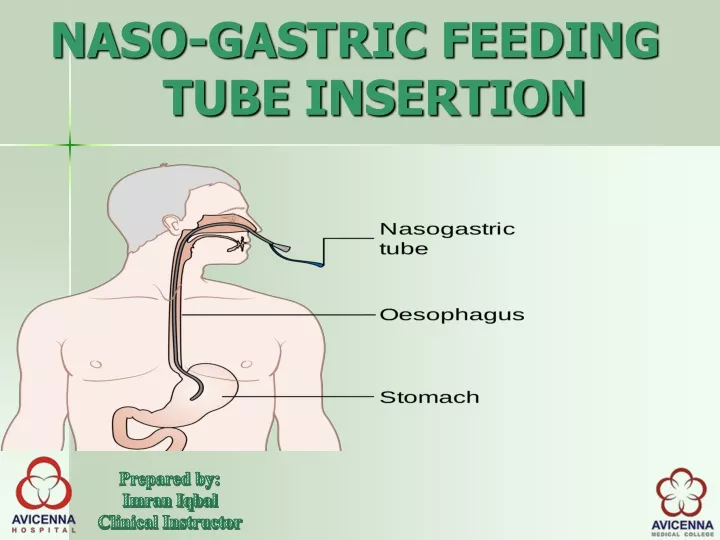
NASO-GASTRIC FEEDING TUBE INSERTION Prepared by: Imran Iqbal Clinical Instructor
DEFINITION • Nasogastric intubation is a process involving the insertion of a plastic tube (nasogastric tube or NG tube) through the nose, past the throat, and down into the stomach.
PURPOSES • Nasogastric tube is used for: • Feeding • Administering drugs • Administering oral agents such as activated charcoal. • To treat life threatening eating disorders • Nasogastric aspiration
PURPOSES • Gastric Lavage • Pre Operatively (Anaesthesia) • Obtaining gastric samples for analysis • Continuous drainage of stomach contents
PURPOSES • Administration of radiographic contrast to the GI tract • Evaluation of upper gastrointestinal (GI) bleeding (i.e, presence, volume)
DIFFERENT SIZES • New born • INFANT SIZES • PAEDIATRIC SIZES • ADULT SIZES
SIZES FOR NEW BORN 4 Fr 5Fr 6 Fr
INFANT AND CHILDREN UP TO 5 YEARS 7 Fr (Orange) 8Fr(Blue) 10 Fr (White)
CHILDREN ABOVE 5 YEARS 12 Fr (White) 14 Fr (Green)
NGT SIZES FOR ADULTS 16 Fr (Orange) 18 Fr (Red) 20 Fr(Yellow)
EQUIPMENTS NG Tube – Appropriate size Disposable gloves Lubricant and gauze – to lubricate NG tube tip Disposable bowl – in the event of vomiting Paper towels – to allow patient to wipe around their mouth if needed Catheter tip syringe (Feeding Tube)
EQUIPMENTS pH testing strips – to assess pH of aspirate Tape / dressing to secure NG tube Glass of water for the patient (if swallow is deemed safe) Local anaesthetic spray – if available Stethoscope Torch Megal’s forceps
PROCEDURE 1. Position the patient sitting upright with their neck straight
LUBRICATE THE DISTAL END Lubricate the tip of the NG tube
PROCEDURE Insert the NG tube in through a nostril – warn the patient prior
PROCEDURES Gently advance the NG tube through the nasopharynx
Ask the patient to take some sips of their water and swallow This can help facilitate the advancement of the NG tube However avoid giving patients a drink if their swallow is deemed unsafe
PROCEDURE This is often the most uncomfortable part for the patient, so don’t go too slowly If resistance is met, rotating the NG tube to 180 degrees can help. however DO NOT force the NG tube If the patient is becoming distressed or gagging, Pause to allow the patient to relax It’s useful to look inside the patient’s mouth intermittently to ensure the NG isn’t coiling in there
pH CHECKING Aspiration of NG tube 1. Attempt to aspirate gastric contents: If aspiration is successful, test the pH (if pH is <4 this suggests correct placement) If aspiration is unsuccessful or the pH is >4 the patient will require a chest x-ray (CXR) Some hospitals require a CXR regardless of pH, so check your local guidelines
SOON AFTER THE INSERTION After the tube is inserted, remove the tube right Away if: coughing Gagging Sneezing Vomiting Wheezing Changing colour
Cannot catch a breath change in respiratory rate change in oxygen needs Decrease in pulse oximeter readings Increased restlessness Unexplained irritability, discomfort, or abdominal pain Cannot talk or change in the quality of cry or you see the tube coming out of the mouth
PATIENT’S EDUCATION To complete the procedure 1. Explain to the patient that the procedure is over 2. Reassure that the NG tube will become more comfortable over the next few hours 3. Offer patient paper towels to clean their face and nose
DOCUMENTATION • Document clearly the procedure of NG tube placement: • Your full name and medical grade • Procedural details and any complications • CXR details if used – e.g. NG tube visible sitting below the left hemidiaphragm • Outcome – e.g. “SAFE to commence feeding” • Your signature, and registration number
COMMUNICATION TEAM MEMBER Inform nursing staff that the NG tube is inserted and safely positioned
TUBE REPLACEMENT • The use of a nasogastric tube is suitable for enteral feeding for up to six weeks. • Silicone feeding tubes are unaffected by gastric acid and can therefore remain in the stomach for a longer period • (6 weeks) • PVC tubes, which can only be used for up to two weeks.
KEEP HEAD SIDE ELEVATED UP TO 60 DEGREE FOR AT LEAST 30 MINS
DOCUMENTATION 1-Amount of aspiration 2-Type and amount of diet given 3-Any complaint during feeding 4-Your Signature and ID number
GASTRIC LAVAGE DEFINITION: Removal of potentially toxic contents from a patient’s stomach. INDICATIONS: Strongly consider nasogastric lavage in a patient who has taken an overdose of drugs that are particularly toxic. Suspected extreme doses associated with high morbidity/mortality and do not have easily available and effective antidotes.