Download
1 / 25
250 likes | 352 Views
ADHD IN CHILDHOOD. Marina Danckaerts, UPC-K.U.Leuven. Highlights in Psychiatry, 2007. Disclosure. Have served in Advisory Boards of Cephalon, Janssen, Lilly, Medice, Novartis, Pfizer, UCB Have received support for public speaking from Astra-Zeneca, Janssen, Lilly, Novartis, UCB

E N D
ADHDINCHILDHOOD Marina Danckaerts, UPC-K.U.Leuven Highlights in Psychiatry, 2007
Disclosure • Have served in Advisory Boards of Cephalon, Janssen, Lilly, Medice, Novartis, Pfizer, UCB • Have received support for public speaking from Astra-Zeneca, Janssen, Lilly, Novartis, UCB • Have received research support from Janssen, Lilly
Highlights in ADHD research in childhood and adolescence • Linking neuroscience to neuropsychology and to behaviour • Gene-environment interactions • Treatment guidelines • Medication side-effects • Long term treatment outcome • Early psychosocial treatment • Other treatments
Neuroscience-neuropsychology-behaviour Casey ea 2007, Curr Opin Neurol; Swanson ea 2007, Neuropsychol Rev • ADHD = disorder of self-control • Prefrontal cortex is central in regulating behaviour (top-down), but subcortical and posterior systems are critical in signaling this system to engage (bottom-up) • Control functions may function well when they are “on-line”, but may not be brought on-line when needed • Most puzzling: • variability in performance • heterogeneous findings MRI and fMRI studies systematically show abnormalities in prefrontal cx, n.caudatus, cerebellum & parietal cx
Neuroscience-neuropsychology-behaviourDevelopment Increased long-range and decreased short range connectivity with age Fair et al., 2007 Delay or interruption in these developmental processes might be associated with cognitive deficits in ADHD.
Neuroscience-neuropsychology-behaviourDevelopment Possession of the DRD4 7-repeat allele was associated with a thinner right orbitofrontal/inferior prefrontal and posterior parietal cortex. Participants with ADHD carrying the DRD4 7-repeat allele had a better clinical outcome and a distinct trajectory of cortical development with normalization of the right parietal cortical region. Shaw ea 2007, Arch Gen Psychiatry
Neuroscience-neuropsychology-behaviourDevelopmental theories Casey ea 2007, Curr Opin Neurol; Tripp & Wickens 2007, Eunethydis Meeting • Model: dopamine reinforcement learning ADHD Normal development Learning to “expect” Reward dependent
Highlights in ADHD research in childhood and adolescence • Linking neuroscience to neuropsychology and to behaviour • Gene-environment interactions • Treatment guidelines • Medication side-effects • Long term treatment outcome • Early psychosocial treatment • Other treatments
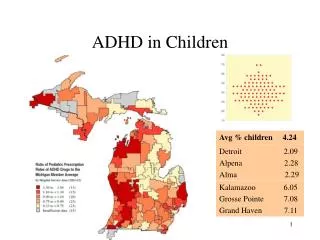
Heritability 0.6-0.9 Meta-analysis: DRD4: 7-repeat allele ~ ADHD DAT1: less reliable association Prenatal smoking, alcohol Family adversity Low birth weight, prematurity Low-level Lead exposure Genes / Environment Li ea 2006, Hum Mol Genet Nigg ea 2007, Biol. Psychiatry
Gene-environment interactions • Genotype as a resilience factor in the presence of psychosocial adversity (Nigg ea 2007) • DAT1 only associated with ADHD in those exposed to prenatal smoking (Kahn ea 2003; not confirmed by Langley ea 2007) • Stronger association with DAT1 when mother consumed alcohol during pregnancy (Brookes ea 2006) • DRD2 x marital status interaction (Waldman, 2007)
Highlights in ADHD research in childhood and adolescence • Linking neuroscience to neuropsychology and to behaviour • Gene-environment interactions • Treatment guidelines • Medication side-effects • Long term treatment outcome • Early psychosocial treatment • Other treatments
ADHD Treatment Guidelines EU Guidelines US Guidelines • 1997: AACAP (American Academy of Child and Adolescent Psychiatry, J Am Acad Child Adolesc Psychiatry 1997) • 2000: Texas Children’s Medication Algorithm (Pliszka GR et al. J Am Acad Child Adolesc Psychiatry 2000) • 2000: NIH (National Institute of Health, J Am Acad Child Adolesc Psychiatry, 2000) • 2001: AAP (American Academy of Pediatrics, Pediatrics 2000) • 2006: Revision of Texas Children’s medication Algorithm (Pliszka GR et al. J Am Acad Child Adolesc Psychiatry 2006) • 2007: AACAP(American Academy of Child and Adolescent Psychiatry, J Am Acad Child Adolesc Psychiatry) • 1998: Clinical Guidelines for hyperkinetic disorder (Taylor E et al.Eur Child Adolesc Psychiatry 1998) • 2004: European Clinical Guidelines for hyperkinetic disorder – first upgrade (Taylor E et al.Eur Child Adolesc Psychiatry 2004) • 2006: NICE guidelines (www.NICE.org.uk) • 2006: Long-acting medications for the hyperkinetic disorders – a systematic review and European treatment guideline (Banaschewski T et al.Eur Child Adolesc Psychiatry 2006)
Treatment Guidelines • Growing armamentarium • More evidence based • Growing literature on side-effects • Choice stimulants and non-stimulant Effect gradual over weeks Long-lasting effect May be preferred in comorbid cases with tics, anxiety, risk of substance abuse Effect size 10% larger Full effect after days Lower cost Spencer ea 2007, Geller ea 2007, Kelsey ea 2007, ESCAP Posters
Highlights in ADHD research in childhood and adolescence • Linking neuroscience to neuropsychology and to behaviour • Gene-environment interactions • Treatment guidelines • Medication side-effects • Long term treatment outcome • Early psychosocial treatment • Other treatments
Medication Side-effects/Safety • 2006: FDA data review adverse events to ADHD medications (Mosholder 2006) • 2006: postmarketing safety data review (Gelperin, 2006) • Box warning US: Atx: suicidal thinking in 4/1000 versus 0 in placebo • 2006: FDA data review on sudden deaths in patients using stimulants (Villalaba, 2006) • 20 on amphetamine, 14 on MPH: does not exceed base rate of sudden death in general population • Advise: not to be used in children with pre-existing cardio-vascular risk without cardiologist’s advise Conclusion: closer monitoring
Highlights in ADHD research in childhood and adolescence • Linking neuroscience to neuropsychology and to behaviour • Gene-environment interactions • Treatment guidelines • Medication side-effects • Long term (treatment) outcome • Early psychosocial treatment • Other treatments
MTA: NIMH landmark study Month 0 14 24 36 22-m Follow- up After Treatment 10-m Follow- up After Treatment 14-m Treatment Stage Medication Only 144 Subjects Random Assignment Psychosocial (Behavioral) Treatment Only 144 Subjects Combined Medication & Behavioral Treatment 145 Subjects 579 ADHD Subjects Community Controls No Treatment from Study 146 Subjects Follow-up (24 m) Mid- treatment (9 m) End Treatment (14 m) 36 m FU Early Treatment (3 m) Recruitment of LNCG Cohort
MTA: 14-month outcome Teacher SNAP-Inattention Average Score Assessment Point (Days)
MTA: 36 month Follow-Up Influential study, but hard to interpret at this point in time ! Stop study Tr. Initial treatment does not seem to make a difference. All did better. Continuous Med (> 50% of days) versus non-continuous Med : no difference Jensen ea 2007
Outcome research All children had 3y.multimodal treatment between 6-12y
Preschool identificationPoor outcome At 11-13y and 12-14y, fewer children with preschool ADHD were well-adjusted (17,7%) than controls (71.4%) Medication works less well in preschoolers: PATS-study: 21% normalized with medication, 13% with placebo (Daley, 2007, Eunethydis)
Highlights in ADHD research in childhood and adolescence • Linking neuroscience to neuropsychology and to behaviour • Gene-environment interactions • Treatment guidelines • Medication side-effects • Long term treatment outcome • Early psychosocial treatment • Other treatments
Psychosocial treatmentParent Management Training Pelham ea, in press; VandenOord ea, in press; Jones ea 2007; • New Forest Parent Training for preschool ADHD children (UK) • Positive Parenting Plan (Triple P- US) • Incredible Years (UK) All work (3-P somewhat less), so far no external validation (only parent ratings) Self-administration packages
Other therapies • EEG-biofeedback (Hirschberg, 2007) • Food supplements (Johnson ea 2007) • Cognitive rehabilitation
Conclusions Genes/Environment Neuro-anatomy/ Brain development Neurophysiology/Neuropsychology Behaviour Treatment Outcome