Download
1 / 33
330 likes | 334 Views
Learn about the challenges and outcomes of hoarding behavior on an individual and community level, as presented by experts in the field. Discover the history of the West Hollywood Hoarding Taskforce and how it works to prevent fires and maintain a healthy environment. Explore the different types of hoarding behavior, co-morbid problems, and the DSM-V diagnosis for hoarding disorder.

E N D
Presented by • Marina Berkman, M.S., MFT, Director of West Hollywood Comprehensive Service Center • Sheila Richman, LCSW, Mental Health Social Worker
Overview • Description of the Two Levels • West Hollywood Hoarding Taskforce • Overview of Hoarding Behavior • Case Studies • Aspects of Case Management • Outcomes
Challenges We Encountered Individual Level • Health complications • Possibility of eviction • Danger of being trapped • Social isolation Community Level • Fire hazard • Structural damage • Public health
History of the Taskforce Creation • After two house fires caused by accumulation of combustive materials • which occurred in 2009, the City of West Hollywood created Hoarding • Taskforce. The goal was to prevent such fires in the future, assure safety • of the residents and maintain a healthy environment. Jewish Family Service • was invited to join the Taskforce. Who is on it? • Social Services Department • Rent Stabilization and Housing Department • Code Compliance Division • City Attorney • JFS social workers
… and How It Works • Referrals received by the City of WH are made by • the landlords, building managers, neighbors, friends, etc. • New cases are discussed at the monthly Taskforce meetings • Strategy of approaching a case is developed by the members • Coordination of efforts between the social worker and • appropriate City staff • Follow up discussion and further strategic planning takes place • at the monthly meetings
Types of Hoarding Behavior • Saving (sentimental, instrumental, intrinsic) • Acquisition (buying, getting free stuff such as • giveaways or picking through garbage) • Clutter/disorganization
Types of Saving Behavior • Sentimental – “This represents my life” or “This item belonged to my grandmother” • Instrumental – “I can use it to repair something” or “It will be donated and can be useful to poor people” • Intrinsic – “This is too beautiful to be thrown away, I need to keep it”
Compulsive Acquiring • Compulsive Buying - retail/discount - web shopping • Compulsive Acquiring of Free Things - free samples - giveaways - trash picking • Stealing/Kleptomania
Clutter/Disorganization Reasons: • Fear of putting things out of sight • Indecisiveness • Churning • Fear of making wrong decision • Inability to categorize belongings
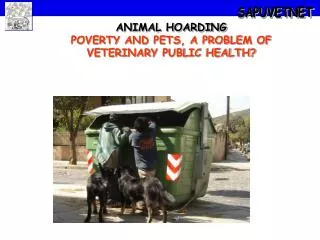
Animal Hoarding • Accumulation of more animals than a typical pet owner, not a breeder • Failure to provide adequate facilities for the animals; overcrowded or unsanitary living conditions; inadequate veterinary care, poor nutrition, animals unhealthy • Reluctance to place animals in others’ care (Patronik, Lear, & Nathanson, 2006)
Demographics • 2% to 5% of general population • Range from 1 in 50 to 1 in 20 • Early adolescence- age 13 • Present for treatment- age 50 (average) • More common in men • Women seek treatment more often • Peak age- 65 to74 (Dong et al., 2012)
Prevalence of Co-morbid Problems • Major Depression - 57% • Social Phobia - 29% • GAD - 28% • ADHD - 28% • OCD - 17% • Specific Phobia - 12% • PTSD - 6% • Dysthymia - 4% • Panic - 2% • None - 8% (Frost, Steketee, Tolin, & Brown, 2011)
DSM-V Diagnosis Hoarding Disorder Diagnostic Criteria 300.3(F42) A. Persistent difficulty discarding or parting with possessions, regardless of their actual value. B. This difficulty is due to a perceived need to save the items and to distress associated with discarding them. C. The difficulty discarding possessions results in the accumulation of possessions that congest and clutter active living areas and substantially compromises their intended use. If living areas are uncluttered, it is only because of the interventions of third parties (e.g., family members, cleaners, authorities). D. The hoarding causes clinically significant distress or impairment in social, occupational, or other important areas of functioning (including maintaining a safe environment for self and others). E. The hoarding is not attributable to another medical condition (e.g., brain injury, cerebrovascular disease, Prader-Will syndrome). F. The hoarding is not better explained by the symptoms of another mental disorder (e.g., obsessions in obsessive-compulsive disorder, decreased energy in major depressive disorder, delusions in schizophrenia or another psychotic disorder, cognitive deficits in major neurocognitive disorder, restricted interests in autism spectrum disorder). Specify if: With excessive acquisition With good or fair insight With poor insight With absent insight/delusional beliefs
Challenges of Dealing with Hoarding Behavior • Resistance to accept help • High cost of cleaning • Uselessness of forceful cleaning • Necessity to follow up
Barriers to Accepting Services General Challenges • Perfectionism/ Excessive focus on details • Decision-making difficulties (core feature of HD) • Disorganization • Lack of insight
Course of Hoarding Emotional & Behavioral pattern of procrastination & avoidance Difficulty regulating emotions May be precipitated by loss Progressive Little evidence of material deprivation
Creative Reasons to Avoid Disposal • It is valuable • It is vintage/antique • It needs to be fixed first…… • I will when I feel better • I need to sort through first • I don’t know where to start • The weather is too hot…..or too cold • I am in too much discomfort • This item I might need • This was given to me by someone special/mother/friend, at a special event, etc. • I need this info. and will file this later • The garbage bins can’t hold all of it • I need to find the right person to give this to… • I would be wasting if I got rid of this… • I will find a new use for this….. • If I get rid of or file it, I will forget about it • I haven’t read that article, paper, mail circular yet, so I can’t get rid of it
Parameters Accessibility of doors & windows 24 inch ceiling clearance 36 inch pathways Clearance of oven & stovetop Accessibility of kitchen sink Clearance of heating units Disposal/Adequate storage of flammable materials Accessibility of bath/shower
Vignette # 1 Client X • Caucasian widower, age 76 • Referred by West Hollywood City Hall • Residing in one bedroom apartment for 35 years • Clutter Image Rating Scale: 8 • Un-medicated Type 2 diabetic, macular degeneration, peripheral neuropathy • 4 months to enter home • Adamant refusal of cleaning • Moved to Assisted Living after building was sold • DX- Hoarding Disorder w/excessive acquisition w/absent insight/delusional beliefs
Vignette # 2 • Client Y • Caucasian widower, age 82 • Referred after a fall by Fire Dept. and WH Code Compliance • Imminent fire danger • Extremely reluctant/anxious at prospect of home visit • Motivated by fear of eviction • W/client’s participation, 41 hours of cleaning & sorting • Currently safe & accessible by bare minimum standards • Ongoing monitoring/case management • DX- Hoarding Disorder w/excessive acquisition • w/poor insight
Aspects of Case Management • Establishing rapport • Usage of harm reduction method • Developing motivation for cleaning • Getting agreement from a client to start cleaning • Coordination of cleaning with the homemaking agency • Providing on-going services after initial stage is over
Aspects of Case Management #2 Majority of WH clients refuse/decline assistance with cleaning. One of the aspects of case management is to lower the barriers in accepting services. Harm Reduction principles are used to overcome the challenges of this task. Principles of Harm Reduction (adapted for WHHTF) • Do no harm • Do not focus on stopping ALL hoarding behavior • Accept that change comes slowly because: - behavior is long ingrained - with time has come accrual of phenomenal number of objects
Aspects of Case Management #3 Developing Motivation in the Client - Increasing Confidence • Stressing health and safety first • Relating previous successes to ability to make progress in this area • Assisting in changing beliefs and meanings of possessions • Balancing tasks while maintaining trust and rapport • Avoiding an over-focus on discarding • Organizing a plan for sorting (keep, discard, donate, later) Motivational Interviewing - Increasing Insight • “How has this affected you?” • “Has your ability to socialize, have family/friends over been impacted?” • “What would your life be like without the clutter?”
Vignette #3 Client Z • Caucasian widower, age 87 • Referred for assistance with his wife • 6 months to allow home visit • Home visit revealed clutter level 8-9 • Daughter had given up • Declined homemaking assistance until hospitalization • Motivated to return to apartment • Relationship/rapport with SW allowed cleaning • Gentle demeanor, patience & persistence of provider • Environment safe, clean & habitable • Daughter re-established connection • Client: “It’s paradise.” • DSM-5 diagnosis: Hoarding Disorder w/Poor Insight
Outcomes West Hollywood Hoarding Task Force in Numbers • 11/22/2010 through 01/06/2015 • 59 referrals to Task Force • 30 of those referred to Jewish Family Service • 25 stabilized • 4 declined service • 1 in progress
References Dong, X. Q., Simon, M.A., Mosqueda, L., Evans, D.A. (2012). The prevalence of elder self-neglect in a community dwelling population: Hoarding, hygiene, and environmental hazards. Journal of Aging and Health, 24, 512-513. Frost, R.O., Steketee,G. (2010). Stuff: Compulsive hoarding and the meaning of things. Boston: Houghton Mifflin Harcourt. Frost, R.O., Steketee, G., Tolin, D., Renaud, S. (2006). Development of an observational measure of hoarding: The clutter image rating. Steketee, G., Frost, R.O. (2007). Compulsive hoarding and acquiring: Therapist guide. Oxford: University Press Tolin, D.F., Frost, R.O., Steketee, G. (2013). Buried in treasures: Help for compulsive acquiring, saving, and hoarding. Oxford: University Press. Tompkins, M.A., Hartl, T.L. (2009). Digging out: Helping your loved one manage clutter, hoarding and compulsive acquiring. Oakland: New Harbinger Publications.
Acknowledgements Funding for the innovative work with hoarders is provided by the City of West Hollywood. Its commitment to improving the lives of its residents makes a tremendous difference!