Download
1 / 1
30 likes | 156 Views
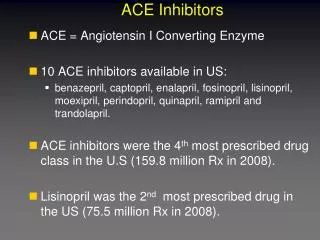
Starting ACE Inhibitors for Heart failure. Patient Presentation. GP. INITIATION NONE of these present- start ACEI Ramipril 1.25mg or Lisinopril 2.5mg consider stopping NSAID or Potassium sparing diuretic. TITRATION Titrate dose slowly by doubling dose fortnightly

E N D
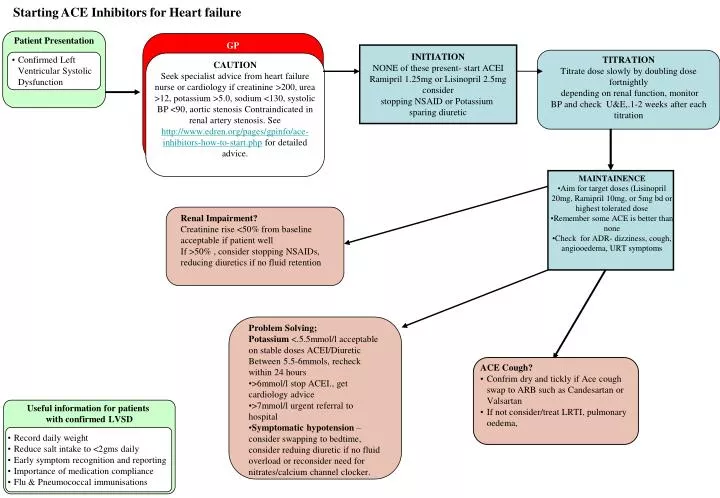
Starting ACE Inhibitors for Heart failure Patient Presentation GP INITIATION NONE of these present- start ACEI Ramipril 1.25mg or Lisinopril 2.5mg consider stopping NSAID or Potassium sparing diuretic TITRATION Titrate dose slowly by doubling dose fortnightly depending on renal function, monitor BP and check U&E,.1-2 weeks after each titration • Confirmed Left Ventricular Systolic Dysfunction CAUTION Seek specialist advice from heart failure nurse or cardiology if creatinine >200, urea >12, potassium >5.0, sodium <130, systolic BP <90, aortic stenosis Contraindicated in renal artery stenosis. See http://www.edren.org/pages/gpinfo/ace-inhibitors-how-to-start.php for detailed advice. • MAINTAINENCE • Aim for target doses (Lisinopril 20mg, Ramipril 10mg, or 5mg bd or highest tolerated dose • Remember some ACE is better than none • Check for ADR- dizziness, cough, angiooedema, URT symptoms Renal Impairment? Creatinine rise <50% from baseline acceptable if patient well If >50% , consider stopping NSAIDs, reducing diuretics if no fluid retention • Problem Solving; • Potassium <.5.5mmol/l acceptable on stable doses ACEI/Diuretic • Between 5.5-6mmols, recheck within 24 hours • >6mmol/l stop ACEI., get cardiology advice • >7mmol/l urgent referral to hospital • Symptomatic hypotension – consider swapping to bedtime, consider reduing diuretic if no fluid overload or reconsider need for nitrates/calcium channel clocker. • ACE Cough? • Confrim dry and tickly if Ace cough swap to ARB such as Candesartan or Valsartan • If not consider/treat LRTI, pulmonary oedema, Useful information for patients with confirmed LVSD • Record daily weight • Reduce salt intake to <2gms daily • Early symptom recognition and reporting • Importance of medication compliance • Flu & Pneumococcal immunisations