Download
1 / 14
230 likes | 565 Views
ExTRACT-TIMI 25. E no x aparin and T hrombolysis R eperfusion for AC ute Myocardial Infarction T reatment – T hrombolysis I n M yocardial I nfarction Study 25. ExTRACT-TIMI 25: Background.

E N D
ExTRACT-TIMI 25 Enoxaparin and Thrombolysis Reperfusion for ACute Myocardial Infarction Treatment–Thrombolysis In Myocardial Infarction Study 25
ExTRACT-TIMI 25: Background • In STEMI patients, prolonged infusion of UFH has not been shown to prevent reocclusion following angiographically successful fibrinolytic therapy • Therefore, current recommendations limit duration of infusion to 48 hours • LMWH vs UFH provides a reliable level of anticoagulation without the need for therapeutic monitoring and with relatively greater proximal inhibition of the coagulation cascade • ExTRACT-TIMI 25 compared LMWH (enoxaparin) and UFH as adjunctive therapy for fibrinolysis in STEMI • Enoxaparin was administered for duration of hospitalization and dosed according to age and renal function LMWH = low-molecular-weight heparin UFH = unfractionated heparin Antman EM et al. N Engl J Med. 2006;354:1477-88.
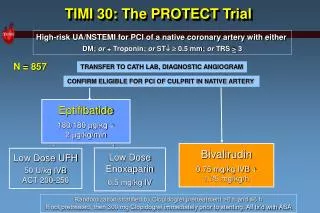
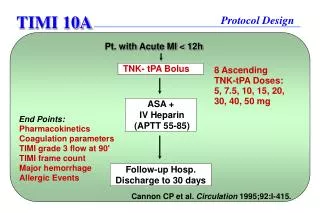
ExTRACT-TIMI 25: Study design N = 20,506 fibrinolytic eligible, STEMI <6 hours Randomized, double-blind, double-dummy ASA 150–325 mg, fibrinolytic (TNK, tPA, rPA, SK) UFH60 U/kg IV bolus, 12 U/kg/h median 2 days Enoxaparin 30 mg IV bolus, 1.0 mg/kg sc q12h* median 7 days Primary end points: Efficacy: Death, MI in 30 days Safety: TIMI major bleeding Net clinical benefit: Death, MI, disabling stroke, nonfatal major bleed, ICH *Aged ≥75 yr: no IV bolus, 0.75 mg/kg sc q12h; CrCl <30 mL/min: ± IV bolus, 1.0 mg/kg sc q24h Antman EM et al. Am Heart J. 2005;149:217-26.Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Medical history and prior treatments Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Baseline characteristics Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Baseline treatment Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Cardiac medications during hospitalization Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Significant reduction in primary end point Death, MI at 30 days 15 UFH 12 9 Enoxaparin End point(%) 6 RR 0.83 (0.77–0.90) P < 0.001 3 0 0 5 10 15 20 25 30 Days after randomization Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Significant reduction in major secondary end point Death, MI, urgent revascularization at 30 days UFH 15 12 Enoxaparin 9 End point(%) RR 0.81 (0.75–0.87) P < 0.001 6 RR (48 hr) 0.88 (0.79–0.98) P = 0.02 3 0 0 2 5 10 15 20 25 30 Days after randomization Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Safety outcomes at 30 days % Favorsenoxaparin FavorsUFH 0 1 2 Relative risk (95% CI) *Primary safety outcome (includes ICH) Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Net clinical benefit at 30 days % Favorsenoxaparin FavorsUFH 0.75 1 1.25 Relative risk (95% CI) Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Overall results • Primary efficacy end pointRate of death or MI was significantly lower with enoxaparin vs UFH (P < 0.001) • Major secondary end pointRate of death, MI or urgent revascularization was significantly lower with enoxaparin vs UFH (P < 0.001) • Safety outcomeRate of major bleeding* in both groups: 2.1% enoxaparin vs 1.4% UFH (P < 0.001) *TIMI criteria Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Summary • In STEMI patients, treatment with enoxaparin throughout the index of hospitalization vs UFH for48 hours demonstrated: • Superior reduction in ischemic events • Increase in episodes of major bleeding • ExTRACT-TIMI 25 results show that treatment strategy with enoxaparin is preferable to the current standard of UFH to support fibrinolysis Antman EM et al. N Engl J Med. 2006;354:1477-88.
ExTRACT-TIMI 25: Clinical implications Nonfatal MI Urgentrevascularization Death Nonfatal major bleeding Antman EM et al. N Engl J Med. 2006;354:1477-88.