Download
1 / 74
880 likes | 1.29k Views
Study Guide for Calcium and Phosphate Metabolism. The most important first messengers for Dental Biochemistry include parathyroid hormone, calcitonin, insulin, and glucagon Name common second messengers and how they operate Define calcium balance

E N D
Study Guide for Calcium and Phosphate Metabolism • The most important first messengers for Dental Biochemistry include parathyroid hormone, calcitonin, insulin, and glucagon • Name common second messengers and how they operate • Define calcium balance • Describe the properties and mechanism of action of parathyroid hormone (PTH) including G-protein function • Review the composition of bone, and know what bone mineral is • What are the two main functions of parathyroid hormone in kidney? • Describe the metabolic activation of vitamin D • What are the actions of vitamin D? • What is osteomalacia? Rickets? Hyperparathyroidism? Pseudohypoparathyroidism? • What is osteoporosis? • Describe physiological ways to establish and maintain maximum bone density • What foods are good sources of dietary calcium?
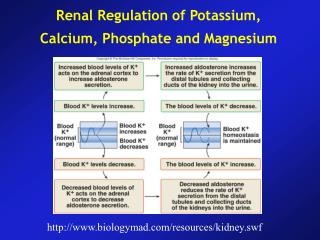
Regulation of Calcium Metabolism • Minerals; serum concentration • Calcium (Ca2+); 2.2-2.6 mM (total) • Phosphate (HPO42-); 0.7-1.4 mM • Magnesium (Mg2+); 0.8-1.2 mM • Organ systems that play an import role in Ca2+ metabolism • Skeleton • GI tract • Kidney • Calcitropic Hormones • Parathyroid hormone (PTH) • Calcitonin (CT) • Vitamin D (1,25 dihydroxycholecalciferol) • Parathyroid hormone related protein (PTHrP)
Sutherland Second Messenger Hypothesis Understand this key concept
Second Messengers Fig. 19-4
Calcium Balance • Intake = output • Negative calcium balance: Output > intake • Neg Ca2+ balance leads to osteoporosis • Positive calcium balance: Intake > output • Occurs during growth • Calcium is essential, we can’t synthesize it
Calcium and the Cell • Translocation across the plasma membrane • Translocation across the ER and mitochondrion; Ca2+ ATPase in ER and plasma membrane
Parathyroid Hormone Structure • Synthesized in the 4 para-thyroid glands • PreProPTH • 115 aa precursor giving a 90 aa prohormone • Cleaved at -6/-7 84 residues in the mature peptide • Regulator of Ca2+ homeostasis
Regulation of PTH Secretion and Biosynthesis • Extracellular Ca 2+ regulates secretion of PTH • Low Ca 2+ increases • High Ca 2+ decreases • Ca2+ also regulates transcription • High levels of 1,25 dihydroxyvitamin D3 inhibit transcription
Calcium Sensing Receptor (CaSR) • Parathyroid chief cells contain a Ca2+ sensing receptor (CaSR) • 7 transmembrane segments (We will see a lot of 7 TM receptors) • mM affinity for Ca2+ • GPCR of the GPLC and GI varieties • Generates inositol 1,4, 5-trisphosphate which increases intracellular Ca2+ • There are two paradoxes • The receptor responds to decreasing concentrations of agonist • Low extracellular Ca2+ increases intracellular Ca2+ • Also found in thyroid C cells (calcitonin), kidney, and brain
Circulating Forms of PTH • Intact, active PTH of 84 aa • Inactive carboxyterminal fragments lack the 1-34 active domain • PTH t1/2 (half life) is 2-3 min • Liver (2/3rds) and kidney (1/3rd) are major sites of fragmentation
Actions of Parathyroid Hormone • Fine tunes Ca2+ levels in blood • It increases Ca2+ • It decreases Pi • Parathyroid hormone acts directly on bone to stimulate resorption and release of Ca2+ into the extracellular space (slow) • Gs protein-coupled receptors in osteoblasts increase cAMP and activate PKA • Inhibits osteoblast function • This occurs when PTH is secreted continuously; the opposite occurs when it is given once daily by injection • Two effects in kidney • Parathyroid hormone acts directly on kidney to increase calcium reabsorption and phosphate excretion (rapid) • Gs protein-coupled receptors • Parathyroid hormone acts on distal tubule • Calcitonin inhibits • Stimulates transcription of 1-alpha hydroxylase for Vitamin D activation in kidney • Vitamin D increases calcium and phosphate absorption
Parathyroid Hormone Receptor • 7 TM • GPCR
Regulation of Adenylyl Cyclase(Fig. 19-11) 7 and 12 TM segments
Cyclic AMP Metabolism (Fig. 19-12) Know each step involved in the generation of cAMP by PTH (words, not structures)
Bone • Inorganic (67%) • Hydroxyapatite 3 Ca10(PO4)6(OH)2 • There is some amorphous calcium phosphate • Organic (33%) component is called osteoid • Type I collagen (28%) • Non-collagen structural proteins (5%) • Proteoglycans • Sialoproteins • Gla-containing proteins (gamma carboxyglutamate) • Phosphoproteins • Bone specific proteins: osteocalcin, osteonectin • Growth factors and cytokines (Trace) • Bone undergoes continuous turnover or remodeling throughout life • About 20% of bone is undergoing remodeling at any one time
Calcium and the Skeleton • A, absorption is stimulated by Vit D; S, secretion • GF, glomerular filtration; TR, tubular reabsorption of Ca2+ is stimulated by PTH
Osteoblasts Bone formation Synthesis of matrix proteins Type I collagen Osteocalcin Others Mineralization Activation of osteoclasts via RANKL production Osteoclasts Bone resorption Degradation of proteins by enzymes Acidification RANK is activated by RANKL, and this leads to cells differentiation to osteoclasts Osteoblast and Osteoclast Function
Bone Remodeling • Osteoclasts dissolve bone • Large multinucleated giant cells • Osteoblasts produce bone • Have receptors for PTH, CT, Vitamin D, cytokines, and growth factors • Main product is collagen • When osteoblasts become encased in bone, they become osteocytes
Osteoclastogenesis: RANKL, RANK, and OPG • Osteoblasts activate osteoclasts, formation of a multinuclear cell • The molecular participants in this pathway are the membrane-associated protein named RANKL (receptor activator of nuclear factor kappa B ligand,) a member of the tumor necrosis factor family of cytokines • Its cognate receptor is RANK; TRAF, TNF receptor associated factors • Mediates activation of NF-kappa-B by unknown mechanism • OPG (osteoprotegerin) is a soluble "decoy" receptor for RANKL • RANKL is expressed on the surface of osteoblastic stromal cells • By binding to RANK, its receptor, on osteoclast precursors, RANKL enhances their recruitment into the osteoclastogenesis pathway in the physiology of bone metabolism • RANKL also activates mature osteoclasts to resorb bone • RANKL is a factor through which osteoblasts regulate osteoclasts, and bone formation is coupled to bone resorption
PTH and Kidney PTH acts on the distal tubule
Calcitonin • Product of parafollicular C cells of the thyroid • 32 aa • Inhibits osteoclast mediated bone resorption • This decreases serum Ca2+ • Promotes renal excretion of Ca2+
Calcitonin • Probably not essential for human survival • Potential treatment for hypercalcemia • 7 transmembrane segment receptor • Stimulates cAMP production in bone and kidney
Proposed Mechanism of Action of 1,25-DihydroxyD3 in Intestine
Vitamin D-dependent Ca2+ Absorption • Duodenum>jejunun>ileum • Absorption is greater at low pH • The pH of the stomach is about 2 • Peak absorption at the beginning of the duodenum
Vitamin D Deficiency: Rickets • Inadequate intake and absence of sunlight • The most prominent clinical effect of Vitamin D deficiency is osteomalacia, or the defective mineralization of the bone matrix • Osteoblasts contain the vitamin D receptor • Vitamin D deficiency in children produces rickets • A deficiency of renal 1α-hydroxylase produces vitamin D-resistant rickets • Sex linked gene on the X chromosome • Renal tubular defect of phosphate resorption • Teeth may be hypoplastic and eruption may be retarded
Vitamin D-Resistant Rickets • Above: Hypoplastic teeth • Below: Minimal caries can produce pulpitis; periapical abscesses are thus common • Lack 1-hydroxylase in kidney • Rx: Respond well to 1, 25-dihydroxyD3
PTHrP; Parathyroid Hormone related Protein • It is synthesized as 3 isoforms as a result of alternative splicing (139, 141, 173 aa) • Can activate the PTH receptor • Plays a physiological role in lactation, possibly as a hormone for the mobilization and/or transfer of calcium to the milk • May be important in fetal development • May play a role in the development of hypercalcemia of malignancy • Some lung cancers are associated with hypercalcemia • Other cancers can be associated with hypercalcemia
Pseudohypoparathyroidism • Symptoms and signs • Hypocalcemia • Hyperphosphatemia • Characteristic physical appearance: short stature, round face, short thick neck, obesity, shortening of the metacarpals • Autosomal dominant • Resistance to parathyroid hormone • The patients have normal parathyroid glands, but they fail to respond to parathyroid hormone or PTH injections • The rise in urinary cAMP after parathyroid hormone fails to occur • The cause of the disease is a 50% deficiency of Gs in all cells • Symptoms begin in children of about 8 years • Tetany and seizures • Hypoplasia of dentin or enamel and delay or absence of eruption occurs in 50% of people with the disorder • Rx: vitamin D and calcium
Pseudohypoparathyroidism Elfin facies, short stature, enamel hypoplasia
Signs and Symptoms of Hypercalcemia • Neurologic • Lethargy, drowsiness, depression, confusion • Can lead to coma and death • Neuromuscular • Muscle weakness, hyptonia, decreased reflexes • Cardiac • Arrhythmias • Bone • Ache, pain, fracture
Causes of Hypercalcemia • Primary hyperparathyroidism • Most people are asymptomatic • Classically affects skeleton, kidneys, and GI tract • Triad of complaints: bones, stones, and abdominal groans • Renal stones are most common single presenting complaint • Usually due to an adenoma (tumor)