Download
1 / 46
460 likes | 658 Views
Follow up of the NICU Graduate. September 14, 2010 Lynn T. Tran, MD and Jeffrey W. Surcouf, MD. Case presentation-O.N. O.N. is a 27 WGA female who was admitted to the NICU for prematurity and resp distress. She comes to you for a F/U clinic visit. What are some things you want to know?

E N D
Follow up of the NICU Graduate September 14, 2010 Lynn T. Tran, MD and Jeffrey W. Surcouf, MD
Case presentation-O.N. • O.N. is a 27 WGA female who was admitted to the NICU for prematurity and resp distress. She comes to you for a F/U clinic visit. • What are some things you want to know? • Maternal labs and prenatal course were noncontributory. • 90 day hospital course notable for • Short duration of intubation • Quick wean to room air • Feeding difficulties • Reflux treated with Ranitidine • Pt discharged home stable on RA with a prescription for Ranitidine and Enfacare/EBM ad lib.
O.N. (cont.) • Previous visits were unremarkable. • Today, she presents to your office 2 months after D/C with the mother complaining that she is not feeding well. • What are some things that you should ask? • Poor feeding (taking appropriate amount with increased effort and spits) • Increased fussiness with feeds • Difficulty sleeping • PE was normal. • What is the diagnosis?
Reflux • Incidence is high in preemies. • Important to distinguish between functional and pathologicreflux
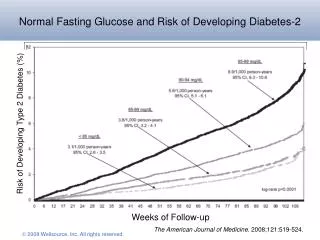
Reflux (cont.) • Frequency: • Mild GER • Term: 40-65% • Course: 55% resolve by 10 mos; 99% by 2 yrs • Preemie: similar to term infants • Pathologic: • Term: 6-7% • Preemies: 3-10%
Reflux (cont.) • Risk factors: • Prematurity • Perinatal depression • Sepsis • Congenital anomalies • Neurologic impairment • h/o ECMO
Reflux (cont.) • Pathophysiology • Relaxation of LES • Sluggish esophageal motility • CNS disorder • Increased abd pressure • Decreased gastric compliance • Anatomic • Decreased acute angle of the esophagus into the stomach • Abnormal diaphragmatic activity • Delayed gastric emptying
Reflux (cont.) • Management: • Mild: • Conservative therapy • Moderate to severe: • Pharmacologic therapy • Histamine-2 antagonists • Ranitidine • Proton pump inhibitors • Omeprazole • Prokinetic • Metoclopramide • Erythromycin First line of tx Not routinely used
Reflux (cont.) • Diagnostic testing • pH probe • Modified barium swallow study • Assesses ability to tolerate different formula consistencies • Endoscopy
O.N. (cont.) • Upon further questioning of the parents, you realize that the dosage of Ranitidine had not been increased for the infant’s weight gain. • Ranitidine dose adjusted with improvement in pt’s sx. • Remember!!! • Course: 55% resolve by 10 mos; 99% by 2 yrs • Try to let infant outgrow the dose and monitor clinically for sx
O.N. (cont.) • During the examination, the mother says, “Enfamil is so much cheaper and easier to obtain. Why is my baby still on Enfacare?” • Your response? • Compared to term formula, postdischarge formulas (Enfacare or Neosure) contains?? • Increased amount of protein with sufficient additional energy • Contains extra Ca, P, Zn • Necessary to promote linear growth • Additional vitamins and trace elements
O.N. (Cont.) • “Ok. Since Enfacare is better for my baby, how long does she have to stay on that formula?” • The AAP recommends: • “The use of postdischarge formula to a postnatal age of 9 months results in greater linear growth, weight gain, and bone mineral content compared with the use of term infant formula.”
O.N. (Cont.) • “What about soy formula?” • The AAP recommends: • Do not use soy formula for: • Preemies weighing < 1800 grams • Prevention of colic/allergy • Infants with cow milk protein allergy
O.N. (cont.) • As the mother is preparing to leave, she mentions, “My best friend says that my baby should be on vitamins. What do you think about that?”
Case Presentation-A.N. • A.N. is a 25 WGA male who was admitted to the NICU for prematurity and resp distress. He presents to your office 1 month after D/C. • What are some things you want to know? • Maternal labs were negative but mother suffered preeclampsia precipitating preterm delivery. • 150 day hospital course notable for • Long duration of intubation • Wean to HFNC then to RA • Apnea of prematurity • Treated with Caffeine • Abnormal sleep study prior to D/C confirming AOP • Pt discharged home stable on RA with a prescription for Caffeine and with an apnea monitor.
Apnea • Apnea is defined by • Cessation of air flow > 20 sec • < 20 sec accompanied by bradycardia or cyanosis • How is this different from periodic breathing? • Periodic breathing is defined as ≥ 3 respiratory pauses of ≥ 3 sec with intervening episodes of respiration < 20 sec • Types • Central • Obstructive • Mixed-most common
Apnea of Prematurity • Incidence inversely related to GA • 100% between 24-29 WGA • 50% between 30-32 WGA • 25% between 34-35 WGA • Usually begins in 1st 2 DOL • When does it end? • By 37 weeks postmenstrual age in infants delivered ≥ 28 WGA • Some infants continue to have apnea beyond 40 weeks postmenstrual age.
A.N. (Cont.) • During the examination, the mother asks, “When can I stop using the Caffeine?” • What are some questions that you should ask? • How often has the monitor gone off? • When it has gone off, what did the baby look like? • How abnormal was the sleep study? • What is the corrected gestational age of the baby? • What dose of Caffeine is the baby receiving?
Caffeine • Mechanism of action: • Stimulatory effects on the brainstem via increasing cAMP levels • May increase diaphragmatic contractility • Dosing: • Loading dose: 20-25 mg/kg IV/PO • Maintenance: 5-10 mg/kg/d IV/PO Q24 • Therapeutic levels: • 5-25 mcg/ml • Side effects: • Tachycardia, restlessness, vomiting • May worsen reflux
Caffeine (Cont.) • Discontinuing Caffeine: • If having events • Consider checking Caffeine level and optimize dose if subtherapeutic • No events • Trial off of Caffeine • Continue on home apnea monitor
A.N. (Cont.) • The mother wants to know how long he has to be on the apnea monitor and states that it is inconvenient and drives her crazy.
Apnea Monitors • In general, when should you be able to discontinue the apnea monitor? • In infants 43 to 46 weeks postmenstrual age or in older infants after 1 month of clinically irrelevant events. • If no recent events, discontinue at least 2-4 weeks after stopping Caffeine. • If the infant had an abnormal sleep study, consider repeating the study prior to stopping the monitor. • This is a clinical decision with no scientific evidence to support the use of sleep studies or home apnea monitoring!
Apnea Monitors (cont.) • Monitors should not be used for healthy preemies with a previous hx of AOP. • Consider monitors for those infants with persistent apnea being sent home on Caffeine or in those infants with isolated, infrequent As/Bs. • Alarm settings: • HR: • Low: 60 – 80 bpm • High: 220 bpm • Apnea: • 20 sec
Home Oxygen Use • Will need concurrent care with Pulmonology to help with discontinuing oxygen
Case Presentation-C.W. • C.W. is a 24 WGA male who was admitted to the NICU for prematurity and resp distress. He presents to Developmental Clinic 3 mos after D/C. • What are some things you want to know? • Maternal labs were negative, but mother presented with preterm labor. • Nearly 1 year hospital course notable for multiple complications particularly • Grade IV bilateral IVH • Pt discharged home on O2 with seizure medications and close neurosurgery follow-up.
C.W. (cont.) • The mother wants to know if it is ok that her baby is not walking as he is now 13 mos old. • Thoughts? • Consider pt’s corrected age • Majority will correct by 1 year of age • However, correction for developmental milestones may be continued until 2 years of age. • What are the risk factors for abnormal development?
Early Interventions • Candidates: • High risk infant • Neurologic condition • IVH • PVL • Seizures • Visual impairment • Hearing loss • At risk infant • BW < 1200g • GA < 32 weeks • Total hospital stay > 25d • APGARS < 5 at 5 min • IUGR • SGA The high risk infant and the at risk infant have the potential for abnormal outcomes…normal HUS does not guarantee normal outcome, nor does abnormal HUS guarantee abnormal outcome. Helping parents understand and cope with this (must be patient) is one of the challenges we face.
Early Intervention • Can be accomplished through • Developmental clinic • School based intervention • Early Steps via parish • Multidisciplinary care • Neurology • PT/OT/Speech • Psychology
Case Presentation-S.W. • S.W. is a 27 WGA male that was admitted to the NICU for prematurity and resp distress. On initial D/C follow up, infant was noted to be gaining weight and doing well. • What are some things you want to know? • Maternal labs were negative, but mother presented with placental abruption. • 2.5 month hospital course • Short intubation period • Prolonged use of supplemental O2 via HFNC • Stage 2 Zone 2 ROP • Multiple courses of Abx due to sepsis • Pt discharged home on RA and PolyViSol with Fe.
S.W. (Cont.) • Upon perusal of the D/C Summary you note: • Newborn screen was drawn on DOL 1 and was found to be normal. • Does this reassure you? • What else should you be asking? • Hepatitis B was given prior to discharge. • BAER was equivocal.
Newborn Screening • New state of Louisiana recommendations • Premature, LBW, or sick infants • Upon admit to the NICU • Hemoglobins, GALT, biotinidase enzymes and provide baseline amino acids and acylcarnitines • 48-72 hours of age • Only if 1st NBS collected < 24 hours of age • 28 days of age or upon discharge • Thyroid, later onset CAH and homocystinuria in preemies
Newborn Screening (Cont.) • Term infants • All should be screened prior to discharge but no later than 7 days of age. • However, risk of false negatives if screened < 24 hrs of age. • Repeat between 1-2 wks of age but no later than 3 wks of age
Newborn Screening (Cont.) • If a specimen is collected after a blood transfusion, repeat testing should be performed: • 3days after transfusion • To detect congenital hypothyroidism, CAH and metabolic disorders detected by MS/MS • And 90 days after last transfusion • To detect sickle cell disease, biotinidase deficiency, galactosemia and cystic fibrosis
Newborn Screening (Cont.) • What about feeds? • Some programs recommend waiting 48-72 hrs after PN • Based on the new recommendations, the timing of feeds does not matter.
Immunizations • Medically stable preemies should receive all routine vaccinations at the same chronologic age as recommended for full term infants.
Immunizations • Palivizumab (Synagis) • 1st dose given during 1st week of November • 5th (last) dose given in March • Indications: • Infants with chronic lung dz ≤ 24 mos of age who receive tx within 6 mos before the start of RSV season (max of 5 doses) • GA ≤ 28 WGA who are ≤ 12 mos of age at start of RSV season • ≥ 28 WGA or ≤ 32 WGA who are ≤ 6 mos of age at the start of RSV season (max of 5 doses) • > 32 WGA or ≤ 35 WGA who are ≤ 3 mos of age or born during RSV season with risk factors (max of 3 doses) • Daycare OR • School aged siblings (< 5 yrs)
S.W. (Cont.) • In addition to Developmental Clinic, what other appointments should you make for this infant? • Audiology • Ophthalmology
Hearing Screen • All infants should receive BAER or OAE in the NICU prior to D/C. • Infants should have repeat screens at 12 months of age if < 32 WGA. • F/U every 6 months after the last hearing screen until 3 yrs of age if at risk for late onset or progressive hearing loss • In utero infection • Hyperbilirubinemia • ECMO • PPHN • Syndromes • Head trauma • Prolonged use of ototoxic medications
Final Thought • Infants are discharged from the NICU with potentially obvious, treatable medical problems. • The parents, however, may be left with less-obvious emotional difficulties due to having an NICU graduate.
FINAL THOUGHT Parents experience, among others: Guilt Fatigue Anxiety and emotional disturbances Financial difficulties…time away from work, medical expenses Marital stress Family stress…what do you tell older siblings? These feelings don’t go away immediately on discharge. Some families cope better than others. As the PCP, it is important to understand these feelings and to support not only the patient, but the family as well. It is important to know where to refer these families if they need more support.
References • http://www.cdc.gov • http://www.dhh.louisiana.gov/offices/?ID=263 • Brodsky, D. and Ouellette, M. Primary Care of the Premature Infant. Saunders Elsevier: 2008. • Chandran, L. and Gelfer, P. Breastfeeding: The Essential Principles. Pediatrics in Review. November 2006: 409-417. • Gomella, T. Neonatology. McGraw-Hill: 2004. • Kleinman, K. Pediatric Nutrition Handbook. American Academy of Pediatrics: 2009. • Vanderbilt, D. et al. The Do’s in Preemie Neurodevelopment. Contemporary Pediatrics. September 2007: 84-92.