Download
1 / 37
380 likes | 1.05k Views
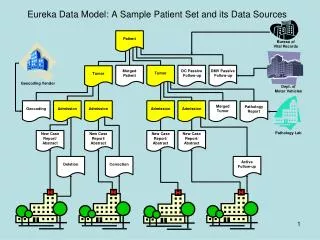
Outline . Case reportPhysiology of bile circulationHigh output biliary fistulaAbdominal bile collection. Case Report. 72 y/o M, left TKR in 91/992/12/1 RUQ pain jaundice cold sweating 1wk ?NTUH ERBil=2.59; Echo: GB CBD stone12/2 ERCP 1(papillotomy lithotripsy)93/3/30 RUQ pain fever chill 1wk4/5 ERCP 2, failed due to papilla Vater stenosis, complicated pancreatitis

E N D
1. High output fistula Ri ???
2. Outline Case report
Physiology of bile circulation
High output biliary fistula
Abdominal bile collection
3. Case Report 72 y/o M, left TKR in 91/9
92/12/1 RUQ pain+ jaundice+ cold sweating 1wk ?NTUH ER
Bil=2.59; Echo: GB+CBD stone
12/2 ERCP 1(papillotomy+ lithotripsy)
93/3/30 RUQ pain+ fever+ chill 1wk
4/5 ERCP 2, failed due to papilla Vater stenosis, complicated pancreatitis & BTI
4. 4/8 high fever persist
4/12 sudden onset of abd pain+ rebounding pain+ impending septic shock
CT: swelling pancreas Echo: dilated CBD & IHD
4/15 PTCD
S/C, U/C: P. aeruginosa
5. 4/26 OP1: cholecystectomy+ choledocholithotomy+ choledochoduodenostomy
5/6 post-OP Cx with bile leakage
5/7 methylene blue intake PO, purplish fluid from RD?NPO
5/10 OP2: jejunostomy for feeding
5/15 OP3: debridement+ abscess drainage? SICU
7. Current problems High output fistula (bile)
Infection
Poor nutrition
Difficult weaning due to metabolic acidosis
8. Case report
Physiology of bile circulation
High output biliary fistula
Abdominal bile collection
9. Bile Content %: Water 97Bile salt 0.7Inorganic salts 0.7bile pigments 0.2fatty acids 0.15lecithin 0.1fat 0.1cholesterol 0.06
500ml/day secreted 80% from liver, 20% from ductule
Stimulated by: bile salts formation (major)organic anions
10. Composition: bile v.s. plasma
11. Bile salts 50% cholesterol degradation to bile salts; 0.2-0.4g/d
3.5g recirculate 6-8/day, 20-30% escape
Major driving force for bile flow and biliary secretion of chol & lethicin
Natural laxatives in colon
12. Bile salts structure
13. Other contents secretin? bile ductular epi? HCO3
Gallbladder: concentrated 10-50X, storage, secret mucus and acidify; evacuation by CCK
14. Enterohepatic circulation
15. Case report
Physiology of bile circulation
High output biliary fistula
Abdominal bile collection
16. Post-choledochostomy acidotic syndrome High-volume biliary output >2L/day
Cause: cholodochocutaneous fistula, T-tube drain, PTCD
Cx: Hyponatremia, dehydration, hypotension, oliguria, metabolic acidosis
Tx: IVF, e- supply, bile refeed, gastric aspiration, internal drainage
17. Bile loss: 1.3-7.7 L/day, almost right after ext. bile drain, persist 2-14 days
Incidence 5% (PTCD in malignant biliary obstruction)
Mechanism: Unknow, hypercholeretic bile acid in serum, biliary hyperplasia, bacteremia, cholangitis
18. Enterocutaneous fistula(ECF) High output> 0.5L/day
Incidence: unclear 80% surgical, 20% spontaneous
Prognostic factor: nutrition, sepsis
Surgical mortality: 6.5-48%
20. Complications Fluid and e- imbalance: NG, H2R antagonist, PPI
Sepsis: most common; due to abscess, 2nd infection of skin, poor nutrition, comorbidity
Malnutrition: 55-90% p�t(+); inadequate intake, hypermetabolism, hypoproteinemia, BW loss >10%; alb> 3.5 mortality 0%alb< 2.5 mortality 42%
21. Management Correct fluid and e- (IVF, correct anemia, e- repletion)
Minimizing malnutrition
Control sepsis (ABx, drain abscess)
Better outcome if do within 1-2 days
Find out the nature: methylene blue, charcol, water-soluble contrast X-ray, fistulogram, CT
22. TPN indications Inability to obtain enteral access
High output fistulas
GI intolerance with enteral nutrition
Multiple unfavorable factors
Not proven well in mortality reduction in ECF, but improve spontaneous closure
23. Effect of TPN Soeters: improve spont closure, but not mortality
Ryan: improved mortality and spont closure
Torres: mean time interval to healing: TPN 20 days, TPN+SS 14 days, closure rate 83%
Ysebaert: TPN+SS, spont closure 83%, duration 11+/-7.9
24. TPN strategy
25. Somatostatin 15 a.a.
inhibit GI secretion, hormone, motility?Reduce fistula output >50% on 1st day
T1/2=1-3 min? rebound hyper-secretion of GH, insulin, glucagon
Inactivated by digestive enzyme
26. Octreotide Synthetic SS analogue
T1/2=2hr, rebound hypersecretion(-)
Prolong GI transit time, decrease endogenous fluid secretions, increased absorption of water and e-
Nubiola-Calonge: ?output in 48h of 70%, ?closure time from 50 to 5-10 days
Martineau: ? output 39-94%, closure 6-13 days after giving
27. Adverse effect Cholelithiasis, biliary sludge formation in <2% for < 1m usage, but >50% for > 1y usage
Nospecific GI symptoms: more often in acromegaly p�t
Infrequent: arrhythmia, hypothyroidism, hypo/hyperglycemia, vomiting, flatulence, abd distension, constipation
28. Clinical usage Start: if 7 days of conservative Tx not ? output
Stop: if no output ? in 48h, or no response after 2-3 wk of Tx
SS: 250ug/h continuous IF
Octreotide: 100ug q8H, sc or IM
29. Conservative failure Operative repair: After 6 wks nutrition support, spont closure doesn�t occurUncontrolled sepsis
Home TPN: poor surgical riskavailable support system? quality of life, ? costTPN long term complication
31. Case report
Physiology of bile circulation
High output biliary fistula
Abdominal bile collection
32. Post-cholecystectomy abdominal bile collections 154 in 179 p�t (86%) drain tube(-)
Bile peritonitis: bile collection+ abdominal pain and tenderness
Bile ascites: bile collection, no S/S
Only 21% bile collection has S/S
Correct Dx initially 23%
34. Reabsorption of bile collection larger than 4cm was rare and unpredictable
35. Predict factor for serious illness:long-term undrained bile (15.4� 19.1 vs 9.2� 10.7) infected bile (45% vs 7%)
Every one with undrained bile was at risk
Suspected whenever persistent bloating and anorexia, failure to recover as smoothly as expected
36. Take home messages Fluid & e- supply, infection control, nutrition support are the mainstay to treat high-output fistula
TPN can improve spontaneous closure rate, but mortality unproven
SS/Octreotide can improve closure time but not spontaneous closure rate
37. Thank you for your attention!!