Download
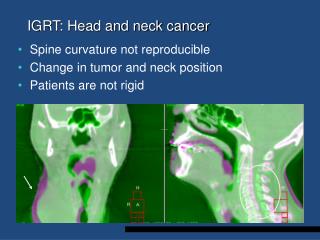
1 / 18
240 likes | 523 Views
HEALTH-RELATED QUALITY OF LIFE IN HEAD AND NECK CANCER SURVIVORS. Department of Otolaryngology-Head and Neck Surgery University of Iowa College of Medicine Iowa City, Iowa . Gerry F. Funk, MD. Iowa Cancer Summit “Maximizing Collaboration Minimizing Disparities” October 17, 2008.

E N D
HEALTH-RELATED QUALITY OF LIFE IN HEAD AND NECK CANCER SURVIVORS Department of Otolaryngology-Head and Neck Surgery University of Iowa College of Medicine Iowa City, Iowa Gerry F. Funk, MD Iowa Cancer Summit “Maximizing Collaboration Minimizing Disparities” October 17, 2008
LONG-TERM HRQOL FOR HEADAND NECK CANCER PATIENTS Collaborators Lucy H. Karnell, PhD Alan J. Christensen, PhD Mark Vander Weg, PhD Amy Trullinger, BA Head & Neck Faculty Henry Hoffman, MD Kristi Chang, MD Nitin Pagedar, MD Rad Oncology Faculty John Buatti, MD Anjali Gupta, MD William McGuiness, MD Medical Oncology Gerry Clamon, MD Head & Neck Nurses Margaret Colwill BSN Helen Stegall BSN Nancy Scroggs • Iowa HNC Outcomes Assessment Program • Iowa HNC Research Consortium
Cancer Survivorship and HNC Patients • Over 50 % of patients treated for cancer, including HNC, in the U.S. will become long-term survivors. • Long-term cancer survivors face physical and psychological treatment effects, recurrence, risk of 2nd primary, co-morbid illnesses, financial-employment-family issues. • HNC survivors are confronted with all the general issues of other cancer survivors including dysfunction of the upper aerodigestive tract. • There are significant knowledge deficits regarding the challenges faced by HNC survivors and an increasing focus on cancer survivorship issues. • NCI Office of Cancer Survivorship, Lance Armstrong Foundation, Center for Disease Control, Institute of Medicine, National Research Council, American Society of Clinical Oncologists. Carvalho et al. Int J Cancer 114:806-816,2005. Trask et al. Am J Prev Med 28:351-356, 2005.References Hewitt M, Greenfield S, Stovall E, Eds. From cancer patient to cancer survivor: lost in transition. National Academies Presses, 2006. CDC. A national action plan for cancer survivorship: advancing public health strategies. Dept of Health and Human Services, 2004. Aziz, Acta Oncologica 46:417-432, 2007. Buckwalter et al. Arch Otolaryngol Head Neck Surg 133:464-470,2007. Karnell et al, Head Neck 28:453-461,2006.
UNIVERSITY OF IOWA HNC OUTCOMES PROGRAM • 1995 Outcomes Assessment Program started • Head and Neck Cancer Specific Function and QOL • Medical Outcomes Study SF-36 • Psychosocial evaluation • Anchor health-state data: demographics, stage, survival, co-morbidity, tobacco & alcohol use, employment,… • Patients • 1462 Enrolled • Analysis based on intent to enroll • Information gathered pre-Rx, 3mo, 6mo, 1yr, yearly • Funding • ACS Seed Grants • ACS Career Development Award, 95-33 • NIH, Office of Cancer Survivorship, RO1,CA 04-003
LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS KEY AIMS • Determine the proportion of 5-year survivors with poor health-related quality of life (HRQOL) outcomes. • Determine differences between short-term (1-year) and long-term (5-year) HRQOL outcomes. • Identify case-mix variables that have predictive value for long-term HRQOL outcomes.
STUDY DESIGN LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS No information • 5-year survivors from an ongoing HNC outcomes study diagnosed between 1/1995-12/2002 • 1201 eligible: 268 refused, 198 not enrolled • 735 enrolled in the outcomes study • 376 dead, 11 refused long-term study, 103 lost to F/U • 245 (20%) provided data for the long-term study • Data collection at pretx, 3, 6, and 9 mo.; 1, 5, and 5+ yr. • Case-mix variables include: age, gender, site, stage, treatment type, social support (Social Provisions Scale), co-morbidity (ACE-27), alcohol & tobacco use, and pain Funk et al, Head Neck 25:561-575,2003. Ware et al, Med Care 1992;30:473-483. Beck et al, Arch Gen Psychiatry 4:561-571,1961. Cutrona et al, JAI Press,1987. Piccirillo JF, Laryngoscope 110:593-602,2000.
The Need For Multi-institutional Data Collection Major Findings STUDY* N, % Original Cohort** Nordgren et al, Int J Rad Onc Biol Phys, 2003 (46, 53%) Nordgren et al, Head & Neck, 2006 (36, 40%) Abendstein et al, Laryngoscope, 2005 (141, 39%) Bjordal et al, Int J Rad Onc Biol Phys, 1994 (204, 24%) Bjordal et al, Oral Oncol Eur J Cancer,1995 (204, 25%) Bjordal & Kassa, Br J Cancer, 1995 (204, 24%) Mehanna et al, Arch OHNS, 2006 (48, 24%) Mehanna & Morton, Clin Otolaryngol, 2006 (43, 21%) Holloway et al, Head & Neck, 2005 (105, CS) Duke et al, Laryngoscope, 2005 (86, CS) Meyer et al, Laryngoscope, 2004 (64, CS) Campbell et al, Arch OHNS, 2004 (62, CS) Zelefsky et al, Am J Surg, 1996 (29, 27%) Terrell et al, Arch OHNS, 1998 (46, 14%) Rogers et al, J Cranio-maxillofac Surg,1999 (38, 17%) Laccourreye et al, OHNS, 2000 (90, ?) Evensen et al, Int J Rad Onc Biol Phy,2002 (67, 15%) Wijers et al, Head & Neck, 2002 (39, ?) Funk et al, AHNS, 2008 (245, 20%) Physical function poor. No substantial clin signif deterioration except dry mouth (1-5yr). No signif change in global QOL for group. Low life satisfaction & general health compared with Age-matched norms. 35% smoking. Pain, cognitive fxn, social fxn, and stage predict psychological problems. Overall life satisfaction decreased over 10 years. Global QOL at 1 year predicted long-term survival. Long-term survivors demonstrated significant aspiration. Personality traits predicted QOL. Poor dental status disrupted global measures of QOL. Global QOL tied much closer to pain & depression than functional status. There is a disconnect between toxicity and QOL. Long-term effects may be related to and predate late effects. No significant change 1 to 5 years. 50% long-term pain. Problems related to dry mouth. * All studies consisted of survivors >5 years after diagnosis. ** CS=convenience sample, ?=unable to determine.
245 patient enrolled in long-term study LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS Substantial co-morbidity Cohort is not dominated by early-stage disease High percentage continuing to use tobacco and alcohol Substantial number of participants with persistent depressive symptoms and pain
LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS Objective 1 Proportion with poor HRQOL 5-year HRQOL outcomes
Objective 2 Change in HRQOL from short-term (1 yr) to long-term (5 yr) LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS 1- vs 5-year HRQOL outcomes a Repeated-measures general linear model tests of within-subject effects B Funk et al, Arch Otolaryngol Head Neck Surg 130:825-829,2004.
Objective 3 Predictors of 5-year HRQOL outcomes LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS Linear regression multivariate analysis
LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS Significant association of pain with long-term HRQOL
LONG-TERM OUTCOMES OF HEAD AND NECK CANCER PATIENTS • We have the largest longitudinal cohort of long-term HNC survivors with HRQOL data. It is dynamic and increasing in size. • Treatment and site-specific analysis • Overall HRQOL measured at 1 year does not show any clinically significant change at 5 years (better or worse) • By 1 year, the acute effects are largely resolved • The long-term effects of HNC treatment are stable • Less than 50% of HNC survivors have a normal eating pattern • A high percentage of HNC survivors have identifiable depressive symptoms • A high percentage of HNC survivors have substantial co-morbid illness • In comparison to age-matched norms, HNC survivors have worse physical and mental health • Pain is long-term and predictive of poor HRQOL. • Long-term survivorship is not an issue confined to early-stage patients.
HNC PATIENTS AS CANCER SURVIVORS • Well over 50% of HNC patients will survive their cancer. • The average age at HNC diagnosis is ~ 64 years and is increasing. • Co-morbid illness will account for ~ 30% of deaths within 5 years of HNC diagnosis. • In the US, the percentage of HNC patients of ethnic minority is increasing. • Patients from lower economic strata are overrepresented among the HNC population. • Rates of second primary cancer and recurrence are high in HNC population. • Unhealthy lifestyles persist after treatment (20% tobacco and >40% alcohol, higher levels of poor nutrition). The percentage of HNC patients who fall into groups at risk for underutilization of necessary health care services is increasing. Hoffman et al, Arch OHNS, 1998 Argiris et al, Clin Can Res, 2004 Sikora et al, Laryngoscope, 2004 Funk et al, Head Neck, 2002 Allison et al, Oral Onc, 2001
HNC PATIENTS AS CANCER SURVIVORS Underutilization of necessary health care services has been identified in colorectal, breast, childhood, and other cancer survivors. There are few published series and conflicting results. General preventive care Recommended cancer screening Provider dependent? Earle et al, J Clin Oncol, 2003 Earle et al, Cancer, 2004 Hewitt et al, J Clin Oncol, 2002 Oeffinger et al, Pediatr Blood Cancer, 2004
HNC Patients as Cancer Survivors and Survivorship Practice Guidelines • “…comprehensive evidence-based guidelines for the care of adult cancer survivors are not currently feasible.” • Comprehensive, evidence based, age- and gender- specific guidelines addressing general health maintenance and cancer screening among HNC survivors are lacking. • NCCN, AHNS – Limited recommendations • General health screening, cancer screening, swallowing evaluation, orodental rehabilitation… T4N2c SCCA Oropharynx Earle CC, J Clin Oncol, 2007
HNC PATIENTS AS CANCER SURVIVORS Cancer and Aging Program Proposal Investigators: Gerry F. Funk, MD Lucy H. Karnell, PhD Alan J. Christensen, PhD Title:Evaluation ofHealth Care Utilization by Head and Neck Cancer Survivors. Specific Aims: 1) Determine the rate of health maintenance interventions, cancer screening interventions, and preventable hospitalizations for ambulatory care-sensitive conditions for head and neck cancer survivors compared to age, race, gender, and geographic location matched controls. 2) Evaluate the influence of age, race, gender, provider specialty, and residence within a poverty ZIP code on health care utilization by HNC survivors.
TALKING POINTS • HRQOL can be improved in HNC survivors through directed interventions. • The overall survival of HNC patients can be improved by improving the global health management of survivors. • Comprehensive, evidence based guidelines for the healthcare of HNC survivors would be helpful. • Specialized services within the University setting AND community resources will be required to accomplish these goals.