Download
1 / 21
210 likes | 325 Views
Frank Wood, Ph.D. Honorary Professor of Behavioural Medicine Nelson R. Mandela School of Medicine Durban, Republic of South Africa and Professor Emeritus Wake Forest University School of Medicine Winston-Salem, NC, USA. Clinical Practice in Brain-Behavior Relationships.

E N D
Frank Wood, Ph.D. Honorary Professor of Behavioural Medicine Nelson R. Mandela School of Medicine Durban, Republic of South Africa and Professor Emeritus Wake Forest University School of Medicine Winston-Salem, NC, USA Clinical Practice in Brain-Behavior Relationships
Clinical Practice in Brain-Behavior Relationships 1. Basic dimensions in brain function. 2. Assessing the strength/weakness profile. 3. Applications to major life issues. 4. Forensic implications.
A. Attentional Style. B. Hemispheric Laterality . C. Dorsal vs. Ventral Stream. D. Episodic vs. Semantic Memory. 1. Basic Distinctions In Brain Function
A. Attentional Style Novelty: Its detection is every brain's goal. To seek or avoid it is every brain's choice. The consequences of novelty are: Arousal Attentional Focus T
Attentional Focus Underfocused: Underaroused and arousal-seeking Broad. Shallow. “Big Picture.” Distractible. Flexible. Innovative. Overfocused: Overaroused and arousal-avoiding Narrow. Deep. Details. Perseverative. Persistent. Predictable. T
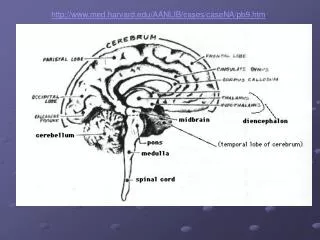
Arousal network is medial and perceptually non-specific; it “tunes” cortical processing. Hyperactivity and Autism. Orbital-medial frontal vs. Dorsolateral frontal. Stimulant medication. Alcohol, etc. Anatomical and Clinical Perspectives on Attention T
1. Neurochemical asymmetries. 2. Approach, Withdrawal, & Reaction time. 3. Language and Spatial Integration. B. Laterality T
Dopamine Target Selection and Field Independence Reward Orientation Neurochemical Laterality T
The right hemisphere specializes in making quick decisions—the kind of decisions, usually to flee, on which survival depends. Thus, the right hemisphere is synthetic; the left, analytic. Approach and Avoidance T
Words are instruments of specificity. Specificity is the essence of language. Syntax is not just coordination of content; it can be directional, i.e. “aim” thought. The right hemisphere is not silent during language. It provides the “melody” of speech, even its accent, and—in a general sense—its context and background. Language and Space T
Even within the left hemisphere, visual stimuli undergo two parallel pathways of processing: Superior parietal-frontal, i.e. “where is it?” & “where are we going?” Temporal, inferior parietal-frontal, i.e. “what is it?” & “what does it describe?” C. Dorsal and Ventral Stream T
Context bound event memory, for episodes of personal experience. Context free memory, for meanings, rules, and procedures. Semantics by definition refers to things true across any episodes. D. Episodic, Semantic Memory T
History is always the most important thing. Often, it's the only important thing. For attentional style, history over-rules any cogniive tests. Whatever the patient's condition, his/her attentional style is the first thing we must know. Psychopathology is all about attention. 2. Assessment: History T
History is also crucial for validating: Memory deficits. These must be understood in the context of daily life, often by report from family or colleague. Symptoms of psychopathology. Cross-contextual manifestations of the patient's problem. 2. Assessment: History T
The simpler they are, the better. It helps if they can sometimes be somewhat criterion-referenced, not only norm-referenced. Story and Word List Recall Drawing and Figure Memory Porteus Mazes and Trailmaking Token and Reporter Tests 2. Assessment: Tests T
Structural Neuroimaging has its limits, too: Undue lesion dependence; undocumented correlations with quantitative findings. Functional neuroimaging, with some exceptions, is not well normed and standardized. Neuropsychological assessment addresses different questions—developmental, competence-based, psychopathological. 2. Assessment: Neuroimaging T
Dementia & Depression: everybody faces it. Low memory can signify depression only. Rehabilitation from Head Injury: treatment means much more than diagnosis. Trauma, Torture, PTSD, and brain atrophy. Academic problems: ADHD, Dyslexia, Psychosis. m 3. Applications to Real Life T
3. Dyslexia N=16 Dyslexia N=15 Controls Childhood scores documented P<.05, corrected for multiple comparisons Bilateral ventral temporo-occipital Left superior temporal T
4. Forensics By definition, forensic work requires making an individual's neuropsychological status relevant to important aspects of life. Test scores and diagnoses will be irrelevant unless they explain real life behavior This principle is equally true for civil and criminal cases. Neuropsychological assessments are often the only way to corroborate life impairment. T
4. Forensics: Assembling the Narrative Age 13 School Years Summer, 2004 Jan 2007 L Selective Language Disability (7th %ile) Left hemi-sphere Under-achievement, Ineffective Coping Frontal Abusive Father VIQ 84, PIQ 99 (13th, 47th %iles) Executive Dysfunction Left & Frontal Hypo-metabolic Left & Frontal
4. Forensics: Some Personal Conclusions Random, explosive violence is frontal; carefully planned violence is temporal. Psychiatric damages are organic; e.g. PTSD; but they can often be suitably managed. Treatment is an issue that cuts both ways. Some verbal ability is required for conciliation and peacemaking—which is a learning process, not just a negotiation. T