Download
1 / 31
320 likes | 519 Views
Antimicrobial therapy Beta-Lactam Antibiotics

E N D
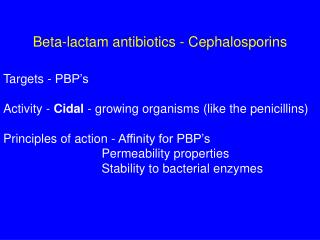
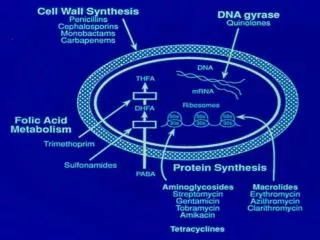
Antimicrobial therapy Beta-Lactam Antibiotics These antibiotics have a B-lactam ring structure and exert a bactericidal action by distrupting cell wall synthesis in rapidly dividing organisms.Generally , they achieve good levels in the lung, kidney , bone , muscle and liver ,and in pleural , synovial , pericardial and peritoneal fluids.They are classified into 8 groups :
1.Natural penicillins:benzylpenicillin,phenoxymethylpenicillin. 2.Penicillinase- resistant penicillins: meticillin, flucloxacillin. 3.Aminopenicillins :ampicillin,amoxicillin. 4.Carboxy-and ureidopenicillins:ticarcillin ,piperacillin. 5.Cephalosporins :1st-4th generation compounds. 6.Monobactams:aztreonam. 7.Carbapenems: imipenem ,meropenem. 8.B-lactamase inhibitors ,e.g. clavulanic acid.
Pharmacokinetics*Not inhibited by abscess environment ( low PH ,low O2 , high protein and polymorphonuclear cells).*Poor penetration to monocytes , low CSF levels except in the presence of inflammation.*Generally safe in pregnancy ( except imipenem/cislastatin).
Adverse reactions *Generalized allergy :0.7-10%. *Anaphylaxis :0.004-0.015% *Infectious mononucleosis :>90% develop a rash if given aminopenicillins. N.B….established penicillin allergy does not imply allergy to other classes,particularly the cephalosporins. *The 2nd and 3 rd generations cephalosporins have a low incidence of allergy and an almost negligible rate of anaphylaxis.
Adverse effects *GI upset ,diarrhea ,and a mild irreversible hepatitis. *Leucopenia , thrombocytopenia and coagulation deficiencies. *Interstitial nephritis and increased renal damage in combination with aminoglycosides. *Seizures and encephalopathy particularly with high doses in the presence of renal insufficiency. N.B…..direct intrathecal injection of a B- lactam is contraindicated.
Macrolide and lincosamide antibiotics Erythromycin:remains the ‘reference’ macrolide antibiotic Pharmacokinetics: -Poorly absorbed orally. -Short half –life(except azithromycin) -High protein binding. -Excellent intracellular accumulation, good CSF penetration.
Pharmacokinetics of lincosamide: -Good bioavailability. -Food has no effect on absorption. -Limited CSF penetration. Adverse effects(both macrolides and lincosamides) *Generally very safe. *GI upset , especially in young adults. *Cholestatic jaundice with erythromycin estolate. *Prolongation of QT interval on ECG ,potential for torsades de pointes. *Clindamycin-diarrhea in 2-30% linked to Cl.difficile.
Aminoglycosides: *Are very effective anti-Gram negative antibiotics. *Are particularly useful where B-lactam or quinolones resistance occurs in health care –acquired infections. Pharmacokinetics: -Negligible oral absorption. -Hydrophilic so excellent penetration to body cavities and serosal fluids.
-Very poor intracellular penetration( except hair cells in cochlea and renal cortical cells ). -Negligible CSF and corneal penetration. -Peak plasma levels 30 minutes after infusion. -Post-antibiotic effect allows once-daily administration ( except in endocarditis , pregnancy , chronic renal disease and ascites ). -Monitoring of therapeutic levels required.
Adverse reactions *Renal toxicity ( usually reversible) , worse with concomitant vancomycin , cisplatin , amphotericin B,contrast media. *Cochlear toxicity( permanent) more likely in order people. *Neuromuscular blockade after rapid intravenous infusion( increased with calcium channel blockers , myasthenia gravis and hypomagnesaemia). N.B…..Aminoglycosides are very effective in Gram-negative sepsis and body fluid infection.
Quinolones *Of these synthetic agents, the early quinolones had purely anti-Gram negative activity, fluoroquinolones ( e.g. ciprofloxacin) have 10-100 times greater activity against Gram-negative organisms , and newer drugs , levo-,moxi-, spar-,gemi- and gatefloxacin, have improved anti –Gram-positive and anti-anaerobic capability. N.B…..These antibiotics may now be used against respiratory pathogens in an empirical manner.
Pharmacokinetics: *Well absorbed after oral administration but delayed by food , antacids,ferrous sulphate and multivitamins. *Wide volume of distribution. *Good intracellular penetration concentrating in phagocytes with high bioavailability. *Tissue concentration twice that of serum.
Adverse reactions *Very rare side-effects. *Rare skin reactions ( phototoxicity). *GI side effects in 1-5% , tremor , dizziness and occasional seizures in 5-12%. *Coadministration with xanthines and theophylines reduces clearance of these drugs so may produce insomnia and increases seizure potential. *CNS effects such as confusion and seizures occur potentially in elderly.
Glycopeptides(vancomycin and teicoplanin) *Vancomycin is effective against Gram-positive organisms and, with teicoplanin, remains useful against MRSA and enterococci. *The inappropriate use of vancomycin should be limited , particularly in the management of Cl. Difficle infections , to prevent further resistance development.
Pharmacokinetics of vancomycin: -Must be given by slow intravenous infusion with good tissue distribution and has a short half-life. -Only enters CSF in the presence of inflammation. Pharmacokinetics of teicoplanin: -Longer half-life allows once-daily dosing. -More lipophilic than vancomycin, with good tissue penetration.
Averse effects of vancomycin: *Histamine release due to rapid infusion produces the ‘ red- man’ anaphylactoid reaction. *Nephrotoxicity enhanced by concomitant aminoglycosides. *Requires therapeutic monitoring. Adverse effects of teicoplanin: *Rash , bronchospasm , eosinophilia and anaphylaxis. *Markedly less toxic than vancomycin ; only requires monitoring in renal impairment.
Folate antagonists -Interfere with the prokaryotic cell metabolism of para-aminobenzoic acid to folic acid. -A combination of two antibiotics ( a sulphonamide and either trimethoprim or pyrimethamine) is most commonly used. N.B…..Co-trimoxazole in high doses ( 120 mg/kg) is the first- line drug for Pneumocystis pneumoniae infection in HIV disease.
Pharmacokinetics: *Well absorbed orally with good bioavailability. *Displace bilirubin from albumin so predispose to kernicterus in infants. *Sulphonamides are hydrophilic , distributing well to the extracellular fluid. *Trimethoprim is lipophilic with high tissue concentrations.
Adverse reactions: *Most are dose- and time- related( therapy for UTI should be no more than 3 days), *Fatal marrow dysplasia and hemolysis in G6PD more common in the elderly. *Skin and mucocutaneous reactions especially common and related to sulphonamide component. *All reactions more common in high- dose therapy in HIV disease.
Tetracyclines *Of this mainly bacteriostatic class , the newer drugs doxycycline and minocycline show better absorption and disribution than older ones. *Are mostly used against Mycoplasma ,Chlamydia and Rickettsia , plus Borrelia and other spirochaetes.
Pharmacokinetics: *Best oral absorption in the fasting state( doxycycline 100% absorbed unless gastric PH rises). *CSF levels increased in chronic inflammation( useful in Lyme disease).
Adverse reactions: *All tetracyclines except doxycycline are contraindicated in renal failure. *Marked effect on bowel flora , causing side-effects of nausea and diarrhoea. *Bind to metallic ions in bones and teeth , causing discoloration(avoid in children and pregnancy). *Phototoxic skin reactions. *Hypernatraemia ( used therapeutically in hyponatraemia)
Chloramphenicol *This potentially toxic antibiotic is bacteriostatic to most organisms but apparentlly bactericidal to H.influenzae ,Strep. Peumoniae ,and Neisseria meningitidis. *It has a very broad spectrum of activity against aerobic and anaerobic organisms, spirochaetes,Rickettsia , Chlamydia and Mycoplasma. *It has quite useful clinical activity against anaerobes such as Bacteroides fragilis.
Pharmacokinetics: *Well absorbed after i.v. or oral dose ( not i.m.).Good tissue distribution and levels. *Good CSF levels. *Crosses placenta and reaches breast milk. *Competes for binding site with macrolides and lincosamides.
Adverse reactions: *Dose- dependent ‘ grey-baby’ syndrome in infants( cyanosis and circulatory collapse due to inability to conjucate drug and excrete active form in urine). *Reversible dose- dependent bone marrow depression( adults) if >4 g per day administered or cuulative dose>25 g. *Severe idiopathic aplastic anaemia in 1:25 000-40 000 treatment regimens ( unrelated to dose , duration of therapy or route of administration)