Download
1 / 39
390 likes | 610 Views
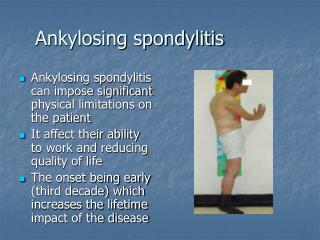
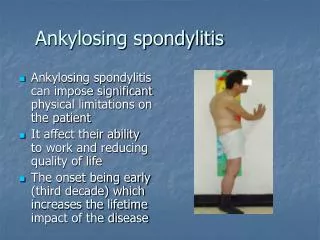
Ankylosing spondylitis. Dr Chris Edwards. Prevalence. Worldwide prevalence up to 0.9% 1 Prevalence varies by population and is closely correlated to prevalence of HLA-B27 2 Prevalence also varies among ethnic groups Male:Female – 5:1 Peak age of onset: 15 – 35 years.

E N D
Ankylosing spondylitis Dr Chris Edwards
Worldwide prevalence up to 0.9%1 • Prevalence varies by population and is closely correlated to prevalence of HLA-B272 • Prevalence also varies among ethnic groups • Male:Female – 5:1 • Peak age of onset: 15 – 35 years 1. Braun et al. Arthritis Rheum 1998; 41: 58-67. 2. Sieper J et al. Ann Rheum Dis 2002; 61 (Suppl. III): iii8-18.
There may also be extra-articular manifestations of AS. • Spinal fracture - most serious complication encountered in AS • Prostatitis is prevalent among men with AS • Long-term disease increases risk of cardiovascular complications • Acute anterior uveitis occurs in 20% to 40% of cases. Other extra-articular manifestations include aortic regurgitation, pulmonary fibrosis, and, among male patients, prostatitis Sieper J et al. Ann Rheum Dis 2002; 61 (Suppl. III): iii8-18.
Etanercept provides a rapid reduction in: • disease activity • Objective functional measures • Work instability This suggests that therapy may be cost effective in terms of work disability Barkham N et al Ann Rheum Dis 2008; 67 (suppl II) : 382
Productivity Costs of ankylosing spondylitis in the USA, The Netherlands, France and Belgium *Adjusted for age and sex. Includes patients with partial work disability who continue in a part-time paid job in The Netherlands and France † in those with a paid job ‡ converted to Euros using 1998 purchasing power parities Sieper J et al. Ann Rheum Dis 2002; 61 (Suppl. III): iii8-18.
Understanding the burden of disease Quality of Life An individuals’ perception of their position in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns World Health Organisation (1995)
Physical function ADL, mobility, physical activity Symptoms Pain, sleep, stiffness, fatigue Global health Social well-being Relationships, opportunities, sexual activity and satisfaction Role activities Employment, household management Emotional well-being Anxiety, control, self-esteem Cognitive function Cognition, concentration, memory Personal constructs Life satisfaction, stigma, Bodily appearance, spirituality Quality of Life
Work disability: AS-specific • Employment rates range 55–85% • 50% of studies report < 70% • Work disability rates range 3–41% • 50% of studies report > 20% • Risk factors: • Age • Disease duration • Physical function** • Pain • Physically demanding jobs • Lower education level Sieper et al, 2002; Boonen et al, 2001
Work disability: AS-specific • Workforce withdrawal • 1st year 5% • 5 years 13% • 10 years 21% • 15 years 23% • 20 years 31% • 3.1x higher than general population Sieper et al, 2002; Boonen et al, 2001
Social well-being • Older studies suggest few problems • Intimate relationships • Men no problems; women less enjoyment (Elst et al, 1984) • Few report marital strain / avoidance (Dalyan et al, 1999) • 27% mild discomfort; 7% severe discomfort (Wordsworth et al, 1986) • Impact on daily life (n 129) - % reporting limitations: • 1% social interactions • 2% communication • 3% normal role activities • 6% leisure activities • (Bakker et al, 1995)
Social well-being: AS and RA • Health status comparison: SF-36 generic health status • AS better Physical health • RA better Mental health • No group differences for: • SF-36: Pain, Physical or Emotional-Role functioning, Social Function, Vitality or General Health • Fatigue (MFI) or Behavioural Coping (CORS) • Work: +ve association with physical health in both groups Chorus et al, 2003
SF-36 scores for patients with RA and patients with AS 100 80 RA male 60 AS male RA female 40 AS female 20 0 Physical Component Mental Component Summary Summary Chorus et al, 2003
Pathogenesis • Immune-mediated, involving: • HLA-B27 • Inflammatory cellular infiltrates • Cytokines such as TNFα and IL-10 • Genetic and environmental factors Sieper J et al. Ann Rheum Dis 2002; 61 (Suppl. III): iii8-18.
AS/SpA: Characteristic Parameters Used for Early Diagnosis Inflammatory Back Pain Symptoms Imaging Lab HLA-B27 ESR/CRP Patient’s history Good response to NSAIDs Family history Rudwaleit M, et al. Ann Rheum Dis. 2004;63:535-43
AS/Axial SpA: Typical Manifestations/Features Positive likelihood ratio (LR+) = sensitivity/(100-specificity) Negative likelihood ratio (LR-) = (100-sensitivity/specificity) Rudwaleit M, et al. Ann Rheum Dis. 2004;63:535-43 Rudwaleit M, Feldtkeller E. and Sieper J. Ann Rheum Dis 2007;. In press.
Ankylosing spondylitis (AS) Undifferentiated SpA Psoriatic SpA Reactive SpA SpA associated with chronic inflammatory bowel diseases Spondyloarthritis - main manifestations • Axial involvement/spinal inflammation • Peripheral arthritis • Peripheral enthesitis Axial SpA SpA subtypes AS
main affection of the spine, entheses, peripheral joints and the eye main symptom: inflammatory back pain 1/3 of patients with severe disease overall prevalence high (0.5%) etiology unknown definite genetic load (new genes !) strong HLA B27 association late diagnosis (5-7 years) reduced quality of life increased risk of unemployment direct/indirect costs Ankylosing Spondylitis: a chronic inflammatory rheumatic disease with debilitating potential 24 years AS 49 years Zink A et al, J Rheum 2000, 2001; Boonen A et al., Ann Rheum Dis 2001, 2002, Ward M et al. J Rheum 2001, A&R 2002
Age at Onset of Symptoms andAge at Diagnosis in AS (DVMB) Time from first symptoms to diagnosis: 5–10 yrs 100 Age at onset of symptoms 80 Age at diagnosis 60 Patients (%) 40 n=1396 20 920 males 476 females Age (yrs) 0 0 10 20 30 40 50 60 70 Feldtkeller E, et al. Z Rheumatol. 1999;58:21-30. Feldtkeller E, et al. Rheumatol Int. 2003;23:61-6.
Differentiating clinical features of IBP in patients < 45 years with chronic back pain ( > 3 months ) • Morning stiffness > 30 min • Improvement with exercise, not with rest • Awakening at 2. half of the night because of pain • Alternating buttock pain * * * * Diagnosis of IBP if 2 / 4 criteria are fulfilled sensitivity 70 % specificity 81 % (AS n = 101; non-AS back pain n = 112) Rudwaleit M et al. A&R 2006
Use of the new IBP criteria as diagnostic criteria in individual patients • Morning stifness > 30 min • Improvement by movement, but not rest • Wakening up in the 2nd half of the night because of pain • Alternating buttock pain Rudwaleit et al. Arthritis Rheum 2006;54:678-81
X-ray evidence of sacroiliitis: a prerequisite for diagnosing AS (modified NY criteria 1984) van der Linden Arthritis Rheum 1984
A role for magnetic resonance imaging in the diagnosis of early sacroiliitis in pondyloarthritides T2 T1 Active sacroiliac inflammation Braun J et al. A&R 1994
The diagnostic value of scintigraphy in assessing sacroiliitis in AS - a systematic literature research • Out of a total of 99 articles about scintigraphy found, 25 were included into the analysis. • Overall sensitivity for scintigraphy to detect sacroiliitis was 52 % for patients with established AS (N= 361) and 49 % for patients with probable sacroiliitis (N= 255). • Sensitivity of scintigraphy in AS patients with inflammatory back pain (indicating ongoing inflammation) was 53 % (N= 112) and in patients with AS and suspected sacroiliitis with magnetic resonance imaging showing acute sacroiliitis (as a gold standard) was 53 % (N=62). • In controls with MLBP specificity was 78 % (N= 60), resulting in LRs not higher than 2.5-3.0. • The data suggest that scintigraphy of the sacroiliac joints is at the most of limited diagnostic value for the diagnosis of established AS including the early diagnosis of probable / suspected sacroiliitis. Song I et al. Ann Rheum Dis. 2008 Jan 29 [Epub ahead of print]
Early back pain cohort: clinical items vs. imaging for the diagnosis of spondyloarthritis n = 69 with IBP < 2 years Heuft-Dorenbosch L et al. Ann Rheum Dis. 2006 Jun;65(6):804-8. Epub 2005 Oct 11
What is helpful for an early diagnosis of AS ? • Screen young patients ( < 45 y) with back pain > 3 months • Ask for inflammatory back pain • Ask for other signs of spondyloarthritis (uveitis, enthesitis) • Do the HLA B27 test • Add imaging when necessary (MRI, X-rays)
AS Measures of Disease Outcome • Bath Ankylosing Spondylitis (BAS) scales • BASDAI – Disease Activity Index • BASFI – Functional Index • BASGI – Global Index • BASMI – Metrology Index • BASRI – Radiographic Index • Other measurement indexes • SF-36 – 36-Item Medical Outcomes Study Short-Form Health Survey • ASAS – Assessments in Ankylosing Spondylitis Working Group Improvement Criteria
Disease Activity Assessment BASFI = Bath Ankylosing Spondylitis Functional Index BASDAI = Bath Ankylosing Spondylitis Disease Activity Index BASMI = Bath Ankylosing Spondylitis Metrology Index ASAS - IC = ASsessment in Ankylosing Spondylitis Improvement Criteria
Visual analogue scale Easy (1) – impossible (10) Mean (VAS) of 10 questions: Putting on your socks or tights without help or aids Bending forward from the waist to pick up a pen from the floor without an aid Reaching up to a high shelf without help or aids (e.g helping hand) Getting up out of an armless dining room chair without using your hands or other help Getting up off the floor without help from lying on your back Standing unsupported for ten minutes without discomfort? Climbing 12-15 steps without using a handrail or walking aid (one foot on each step)? Looking over your shoulder without turning your body? Doing physically demanding activities (eg physio exercises, gardening, sport)? Doing a full day’s activities at home or at work? Bath Ankylosing Spondylitis Functional Index (BASFI) • relate to the functional anatomy of subjects • relate to a subject’s ability to cope with everyday life Calin, J Rheumatol 1994;21:2281-85.
Visual analogue scale (0 – 10 cm) None (1) – Very severe (10) Fatigue - How would you describe the overall level of fatigue/tiredness you have experienced? Spinal pain - How would you describe the overall level of AS neck, back or hip pain you have had? Joint pain - How would you describe the overall level of pain/swelling in joints other than neck, back or hips you have had? Enthesitis - How would you describe the overall level of discomfort you have had from any areas tender to touch or pressure? Inflammation: Duration morning stiffness - How would you describe the overall level of morning stiffness you have had from the time you wake up? Severity morning stiffness - How long does your morning stiffness last from the time you wake up? (scale of 0 to >2 hrs) BASDAI = 0.2 [F + S + J + E + 0.5 (Duration + Severity Morning Stiffness)] Range 0 – 10 Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) Garrett, J Rheumatol 1994;21:2286-91.
Represented as aggregate score (ranging from 0 to 10) using the variables below Bath Ankylosing Spondylitis Metrology Index (BASMI) Jenkinson, J Rheumatol 1994;21:1694-98.
Objectives of disease management • Reduce and/or prevent deleterious effects of: • Inflammation • Ankylosis • Abnormal posture • Aim for: • No or low disease activity (pain, stiffness, MRI, CRP) • Good function, no disability • No structural damage (no growth of syndesmophytes) • Good quality of life • No increased cardiovascular morbidity • Normal life expectancy Dougados M et al. J.Rheumatol 2001;28-62:16-20