Download

1 / 26
260 likes | 366 Views
HL7 UK Conference – October 2006. When is a standard not a standard? The case for unifying LSP approaches to local interfacing. Philip Scott Head of IT Projects & Development Portsmouth Hospitals NHS Trust Co-chair, HL7 UK NHS Implementers group. Why discuss this?.

E N D
HL7 UK Conference – October 2006 When is a standard not a standard?The case for unifying LSP approaches to local interfacing Philip Scott Head of IT Projects & Development Portsmouth Hospitals NHS Trust Co-chair, HL7 UK NHS Implementers group
Why discuss this? • There is an opportunity now to mitigate migration/maintenance problems down the line as CRS deployments progress • There is an opportunity to win over clinical enthusiasm for “yet another system” • If an Enterprise Architecture is being adopted, the “Enterprise” must be complete and not have holes or gaps round the edges • Aim: generate discussion not give answers
Topics • Are standards a good idea? • But we’ve already got standards! • But what about …? • Are there workable solutions? • Questions
Are standards a good idea? • Yes • “Enable clinical semantic interoperability” • Jolly good! • Well that’s alright then • The end • (nearly…)
But we’ve already got standards! • Clinical information content: Snomed CT • Electronic messaging: HL7 v3 • But – what about now?
What about… • Existing non-HL7 message flows supporting operational needs • PMIP and things hanging off it or disguised inside it • Discharge summaries, clinic letters, OOH… • “Legacy” system interoperability • Information flows outside MIM scope
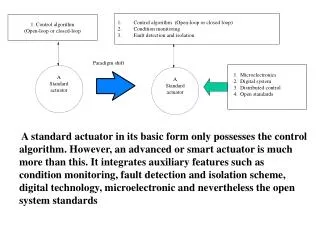
CSC Alliance 1 - NASP Interface – HL7 V3 2 - Existing Systems Interface – HL7 2UK (VA.2) 3 & 4 - Departmental Systems Interface – HL7 V2.3/V2.4
BT Have market forces simplified this already?
Information flows outside MIM scope • HL7 v2 alone does not offer semantic consistency (to say the least) • When you’ve seen one… [laugh now] • “Rampant optionality” • Given Benson’s eq.1: • Therefore:
Information flows outside MIM scope • Other issues of scope: • Realm (home countries, Europe, world) • Service (NHS, social care, police, YOT, housing, education…) • And more immediately for England: • Provider type (NHS, private sector, military) • LSP region (cross-cluster flows) • LSP sub-units (deployment groups ≠ clinical networks, initial “external” visibility = 0)
Information flows outside MIM scope • Current approach is pragmatic commercial reality rather than “ruthless standardisation” • CSC: UK vA.2, v2.3, v2.4 • BT: UK A.2? • Fujitsu: v2.3 • Which v2.3? Which v2.4? Which UK A.2? • Issues: • Maintenance: no re-use possible, upgrades complex • Risk of varying semantics or data quality workarounds • Cross-boundary flows: specialty systems, cancer networks, ISTCs, tertiary referrals, lab to lab
Are there workable solutions? • Use IHE profiles • Develop HL7 v2.5 UK (?) • Change to HL7 v3 (UK?) • Develop Logical Models • HL7 UK NHS Implementers subgroup favoured some sort of logical model to constrain v2 • Certifiable testing (≈ sandpit etc)
And what about…? • “Legacy” systems interoperability • Needed until children grow up (at least) • Eventually true EPR, not for some years • Specialty systems will have to co-exist • Repositories for unsolicited results will have to co-exist (not to mention EDM) • Can we make it easier for clinicians?
Legacy system interoperability • HL7 CCOW • Few applications have it out of the box • Some add-on products offer CCOW-like behaviour/functionality • Front-end integration may be easier in some cases than a messaging interface • Clinicians will bite your hand off for patient context synchronization
Legacy system interoperability • GOSH is procuring a solution via OJEU • PHT is currently procuring via Catalist • LSPs apparently take varying stances (flavours of No) • Is CFH interested…? • Could be low-hanging fruit!
Conclusion • There is an opportunity NOW to mitigate migration/maintenance problems down the line as CRS deployments progress • There is an opportunity to win over HUGE clinical enthusiasm for “yet another system” • If an Enterprise Architecture is being adopted, the “Enterprise” must be COMPLETE and not have holes or gaps round the edges • Discuss…