Download
1 / 28
300 likes | 562 Views
DSM IV CLASSIFICATION SYSTEM PRESENTED BY- Mrs.Shalini Chhabra, Sr.Lecturer Department Of Psychology

E N D
DSM IV CLASSIFICATION SYSTEM PRESENTED BY- Mrs.Shalini Chhabra, Sr.Lecturer Department Of Psychology DAV College For Girls, Yamunanagar
Classification is important in any science whether we are studying plants, planets and people. With an agreed upon classification system we can be confident that we are communicating clearly. If someone says to you “ I saw a coolie running down the street, you probably have an accurate idea of what the coolie looked like- not from seeing it but rather from your knowledge of classification. • In Psychopathology class involves the description of various types of categories of maladaptive behaviour. Classification is necessarily first step towards introducing some order into our discussion of the nature, causes and treatment of such behaviour. It enables communication about particular cluster of behaviour in agreed upon and meaningful way e.g. we can not conduct research on background of causal factor in a given disorder unless with more or less clear definition of behaviour under examination. • FEATURES OF AN IDEAL CLASSIFICATION:-
Granting that all classification system are fundamentally arbitrary, some of them are much better than other in helping us organize and discuss our observations. We take a classification system’s usefulness on its four main features • Reliability:- Reliability is the degree to which a test or measuring device produces the same result each time it is used to measure the same thing.In the case of classification it is a measure of extent to which different observer can agree that a behaviour “fits”a given diagnosis category. • Validity:- Validity refers to the extent to which a measuring instrument actually measures what it claims to measure. In the case of classification validity is determined by whether the diagnostic category tells us something important or basic about the disorder. • 3.Classification system should be more or less permanent. • 4.In the classification system, there should be the
4. In the classification system, there should be the • characteristics of homogeneity in one group of disorder and characteristics of heterogeneity between two group of disorder. • NEED FOR CLASSIFICATION:- • Such systems provide a language with which all mental health professional can communicate. It enables efficient communications e.g. instead of telling all the symptoms of depression, one is able to say only depression to name a particular type of mental disorder. • In order to study the natural history of a particular disorder and develop an effective treatment it is necessary to define the characteristics of disorder and have an understanding of how it is different from other similar disorders to the extent that relationship between diagnosis and treatment has been established for a particular category. The proper diagnosis of a person’s condition can
indicate the most effective treatment. • 3. The ultimate purpose of classification is to develop an understanding of the causes of the various mental disorders. Knowing the causes of the disorder usually leads to the development of an effective treatment. • DSM CLASSIFICATION OF MENTAL DISORDERS:- • History of classification goes back to Hippocrates who classified the mental disorder on the basis of biles. According to him there are three biles in the body. Red, yellow and black. Biles are some enzymes in the body. Red bile is responsible for aggression, yellow for peace and black for severe depression. Official classification of mental disorders first came into the United in 1840. This trend continued in the United States and now a days the most widely used classification scheme in mental disorders in U.S. is Diagnostic and Statistical Manual of Mental Disorders (DSM). There also exists a world wide classification system called ICD which is called a International
Classification of Diseases, which cover all disorders and diseases. Both the Psychiatric Association (APA) and World Health Organization (WHO) have worked closely over the years to ensure compatibility between the classification systems. APA first published DSM I in 1952, DSM II in 1968, DSM III in 1980, DSM III R in 1987 and DSM IV in 1994. DSM IV DSM IV is developed mainly for the purpose for treatment, research and education. This diagnosis manual is constructed and documented on the basis of systematic and explicit process. More than any other nomenclature of mental disorders, DSM IV is grounded in empirical evidence. In DSM IV each of the mental disorders is conceptualized as a clinically significant behavioural or psychological syndrome or pattern that occurs in an individual
and that is associated with present distress or disability or with a significantly increased risk of suffering death, pain, disability or an important loss of freedom. In addition, this syndrome a pattern must not be merely an expectable and culturally sanctioned response to a particular event e.g. the death of loved one. Whatever its original cause, it must currently be considered a manifestation of a behavioural, psychological or biological dysfunction in the individual. Neither deviant behaviour (e.g. political, religious or sexual) nor conflicts that are primarily between the individual and society are mental disorders unless the deviance or conflict is a symptom of a dysfunction in the individual as described above. Multi-axial Assessment:- A multi axial system involves an assessment on several axes, each of which refers to a different domain of information that may help the clinician plan treatment & predict outcome.
There are five axes included in the DSM IV multi axial classification:- Axis I : Clinical Disorders Other Conditions that may be a focus of clinical attention. Axis II : Personality Disorders and Mental Retardation Axis III: General Medical Conditions Axis IV : Psycho-social and Environmental Problems. Axis V : Global Assessment of Functioning AXIS I:-Axis I is for reporting all the various disorders or conditions in the classification except for the Personality Disorders and Mental Retardation (which are reported on Axis II). Also reported on Axis I are other conditions that may be
a focus of clinical attention. When an individual has more than one Axis I disorder all of these should be reported. The principal diagnosis or the reason for visit should be indicated by listing it first. When an individual has both an Axis I and an Axis II disorder, the principal diagnosis or the reason for visit will be assumed to be on Axis I unless the Axis II diagnosis is followed by the qualifying phrase (Principal Diagnosis) or (Reason for Visit). If no Axis I disorder is present, this should be coded as V 71.09. If an Axis I diagnosis is deferred, pending the gathering of additional informational, this should be coded as 799.9 AXIS I Clinical Disorder Other conditions that may be a focus of Clinical Attention
Disorders usually first diagnosed in Infancy Childhood or Adolescence (excluding Mental Retardation, which is diagnosed on Axis II) • Delirium (disordered state of mind), Dementia (incoherent speech), Amnesic and other cognitive disorders • Mental Disorders due to a General Medical condition • Substance related disorders • Schizophrenia and other Psychotic Disorders • Mood disorders • Anxiety disorders • Somatoform disorders • Factitious disorders • Dissociative disorders
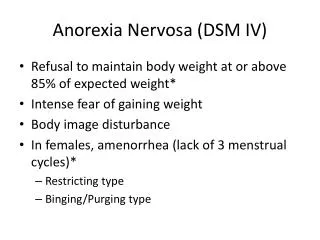
11. Sexual and Gender Identity disorders 12. Eating disorders 13. Sleep disorders 14. Impulse control disorders (not elsewhere classified) 15. Adjustment disorders 16. Other conditions that may be a focus of clinical attention AXIS II: Axis II is for reporting Personality Disorders and Mental Retardation. It may also be used for noting prominent maladaptive personality features and defense mechanisms. The listing of Personality Disorders and Mental Retardation on a separate axis ensures that consideration will be given to the possible presence of Personality Disorders and Mental Retardation that might otherwise be overlooked when attention is directed to the usually more florid Axis I disorders.
If an individual has more than one Axis II diagnosis then all are reported. When an individual has both Axis I and an Axis II diagnosis and Axis II is the principal diagnosis or the reason for the visit, then this is indicated by adding the qualifying phrase,” (Principal Diagnosis” or “Reason for visit” after the Axis II diagnosis). If no Axis II disorder is present, then it is coded as V 71.09. If an Axis II diagnosis is deferred, pending the gathering of additional information, then it is coded as 799.9. • AXIS II • Personality Disorders • Mental Retardation • Paranoid Personality Disorder • Schizoid Personality Disorder • Schizotypal Personality Disorder
4. Anti social Personality Disorder 5. Border line Personality Disorder 6. Histrionic Personality Disorder 7. Narcissistic Personality Disorder 8. Avoidant Personality Disorder 9. Dependant Personality Disorder 10. Obsessive Compulsive Personality Disorder 11. Personality Disorder (not otherwise specified) 12. Mental Retardation AXIS III: Axis III is for reporting current general medical conditions that are potentially relevant to the understanding or management of the individual mental disorder. When an individual has more than one clinically relevant
Axis III diagnosis, all are reported. If no Axis III disorder is present, then that is indicated by the notation “Axis III: None”. If an Axis III diagnosis is deferred, pending the gathering of additional information then this is indicated by the notation “Axis III-deferred”. • AXIS III • General Medical Conditions (with 1CD-9-CM codes) • Infectious and Parasitic Diseases • Neoplasm (growth of tissues in any part of body or tumor) • Endocrine, Nutritional and Metabolic Diseases and Immunity Disorders • Diseases of Blood and Blood forming organs • Diseases of nervous system and sense organs • Diseases of circulatory system
7. Diseases of respiratory system 8.Diseases of digestive system 9. Diseases of genitourinary system 10. Complications of pregnancy, child birth and puerperium (fever due to child birth) 11. Diseases of the skin and subcutaneous tissue 12. Diseases of musculoskeletal system and connective tissue 13. Congenital Anomalies 14. Certain conditions originating in the Prenatal period 15. Symptoms, Signs and ill-defined conditions 16. Injury and Poisoning AXIS IV: Axis IV is for reporting psycho-social and environmental problems that may effect the diagnosis,
treatment and prognosis of mental disorders. A psychosocial or environmental problem may be a negative life event, and environmental difficulty or deficiency, a family related or other interpersonal stress, an inadequacy of social support or personal resources or problem relating to the context in which a person’s difficulties have developed. So called positive stressors, such as job promotion should be listed only if they constitute or lead to problem e.g. when a person has difficulty adapting to the new situation. When an individual has multiple psychosocial or environmental problems in general the clinician note only those problems that have been present during the year preceding the current evaluation. AXIS IV Psychosocial and Environmental Problems
Problems with primary support group • Problems related to the social environment • Educational Problems • Occupational Problems • Housing Problems • Economic Problems • Problems with access to health care services • Problems related to interaction with the legal system/ crime • Other psycho social and environmental problems • AXIS V: Axis V is reporting the clinician judgment of the individual’s overall level of functioning. This information is useful in planning treatment and measuring its impact and in predicting outcome.
This reporting is done using the Global Assessment of Functioning (GAF) scale. The GAF scale reading is done only with respect to psychological, social and occupational functioning. The rating is not done with respect impairment in functioning due to the physical or environmental limitations. In most instances, rating on the GAF scale is done for the current period as it will help in determining the need for treatment or care. In some settings, GAF rating is done both at time of admission and at the time of discharge. In some instances GAF scale may also be rated for other periods e.g. the highest level of functioning for at least a few months during the past year. AXIS V Consider psychological, social and occupational functioning on a hypothetical continum of mental health-illness. Do not include impairment in functioning due to physical or environmental limitations.
Code • Superior functioning in a wide range of activities. Life’s • problems never seem to get out of hand, is sought by • others because of his or her many positive qualities. • No symptoms. • Absent or minimal symptoms. Good functioning in all • areas. Interested and involved in a wide range of • activities, socially effective, generally satisfied with • life, no more everyday problems or concerns. • If symptoms are present, they are transient and
expectable reactions to psychosocial stressors; no • more than slight impairment in social, occupational • or social functioning. • Some mild symptoms or some difficulties in social, • occupational or school functioning but generally • functioning pretty well, has some meaningful inter- • -personal relationship. • Moderate symptoms or moderate difficulties in • 51 social, occupational or school functioning.
Serious symptoms or any serious impairment in • social, occupational or school functioning. • Some impairment in reality testing or communication • or major impairment in several areas, such as work • or school, family relations, judgments thinking or • mood. • Behaviour is considerably influenced by delusions or • hallucination or serious impairment in communication • or judgment or inability to function in almost all • 21 areas.
Some danger of hurting self or others or occasionally • fails to maintain minimal personal hygiene or gross • impairment in communication. • Persistent danger of severely hurting self or others • or persistent inability to maintain minimal personal • hygiene or serious suicidal act with clear expectation • 1 of death. • 0 Inadequate information. • Examples of DSM IV Multi-axial Evaluation
Axis I 296.23 Major Depressive Disorder, Single Episode, Severe without Psychotic Features. 305.00 Alcohol Abuse Axis II 301.6 Dependent Personality Disorder Frequent use of Denial Axis III None Axis IV Threat of job loss Axis V GAF = 35 (current) Evaluation of DSM IV: 1. There are changes in multi-axial system. The childhood and developmental disorders which were on Axis II in DSM III-R are shifted to Axis I in DSM IV.
2. In DSM III-R, Axis IV was for the assessment of severity of psychological stressors. But in DSM IV it is now for the assessment for psychosocial and environmental problems. 3. Axis V is same as in DSM III-R except the scale points have been extended from 90 to 100. 4. Some criteria's of mental disorders have been modified such as the criteria for mental retardation has been modified by including the diagnosis of deficiency of skills. 5. Learning disorders have been introduced in place of academic skill disorders in DSM-III-R. 6. Communication disorders introduced in place of speech disorders in DSM-III-R. 7. Some new disorders have been introduced e.g. feeding disorder, delirium, dementia due to multiple causes, catatonic
disorders due to general medical conditions etc. DSM-III-R disorders deleted from DSM IV are over anxious disorder of childhood, avoidant disorder of childhood, undifferentiated attention deficit disorder, passive aggressive personality disorders. CRITICISM: 1. After so much improvement in DSM IV. Some psychologists shall talk about and doubts regarding the reliability and validity of DSM IV. 2. Some of the psychologists has pointed out that in DSM IV no attention is given to the history and developmental problem of the patient. 3. In DSM IV sometimes the clinicians has to use his impressionistic clinical judgment regarding the client e.g. when a clinician has to decide the severity of particular disorder he has to depend on his own judgment.
4. Some of the criticism focus on the fact that with the DSM classification it is easy to define them in broad category but it is very difficult to go in minute details of particular disorder such sub categories are not mentioned in DSM IV. 5. In DSM IV little importance has been attained to the cause of mental disorders. 6. In DSM classification the clinician has to apply multi-axial System on every patient. It is really very torturous, cumbersome and time consuming. 7. When we apply DSM IV on a particular patient sometimes the symptoms and the criteria do not fit exactly on the patient e.g. if in a particular disorder there are four important symptoms but a patient is showing or exhibiting only three out of them then the doubt arises i.e. whether to put that particular patient in that category or not.
8. In DSM IV there is no provision of putting two disorders together e.g. in day to day life it has been observed that anxiety and depression sometimes they occur together, but in DSM IV there is no such category which is known by the name of Mixed Anxiety Depression disorder but in reality such conditions occur and then the clinician is in the state of uncertainty.
THANK YOU