Download
1 / 59
590 likes | 596 Views
UK donation and transplantation, 2012. Increase deceased donor numbers Reduce end stage organ failure Promote alternative sources / solutions Increase organs utilised per donor Donor optimisation Graft re-conditioning Improve graft longevity. Narrowing the gap.

E N D
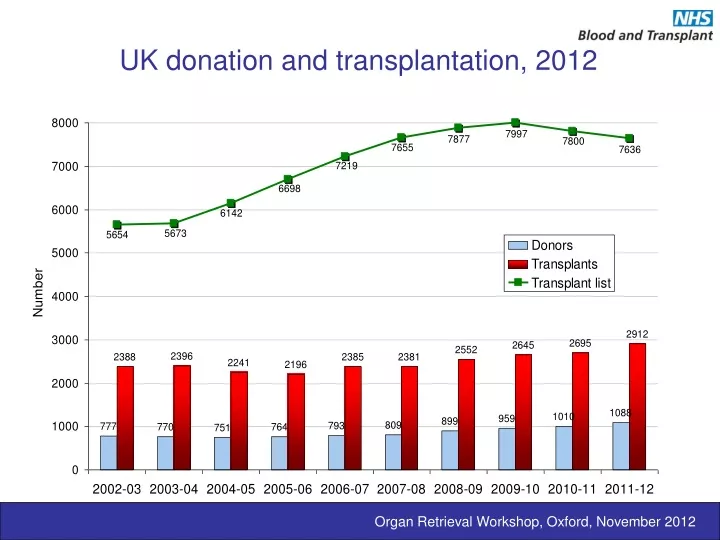
UK donation and transplantation, 2012 Organ Retrieval Workshop, Oxford, November 2012
Increase deceased donor numbers Reduce end stage organ failure Promote alternative sources / solutions Increase organs utilised per donor Donor optimisation Graft re-conditioning Improve graft longevity Narrowing the gap Failure to maximise the gift of donation dishonours both donors and their families Organ Retrieval Workshop, Oxford, November 2012
If the vision is ‘every organ, every time’, the reality is that ‘we lose more than we use’ Heart transplant rates, 2010 Organ Retrieval Workshop, Oxford, November 2012
Phases of graft injury Organ Retrieval Workshop, Oxford, November 2012
Pre-retrieval graft injury Organ Retrieval Workshop, Oxford, November 2012
Organ damage in the DBD donor The brain dead organ donor has a distinct collection of acute physiological disturbances that are almost always correctable Causes of organ impairment • Primary pathology • Chronic co-morbidities • Brain resuscitation therapies • Pathophysiology of brain death • Fluid and electrolyte disturbance • Haemodynamic instability • Neurogenic pulmonary oedema • Endocrine dysfunction • Systemic inflammation Fatty kidney from an obese hypertensive donor Organ Retrieval Workshop, Oxford, November 2012
Cause of death in UK DBD donors % Donor cause of death Organ Retrieval Workshop, Oxford, November 2012
Ages of deceased donors in the UK, 2001-11 Organ Retrieval Workshop, Oxford, November 2012
BMI of deceased donors in UK, 2001-11 Organ Retrieval Workshop, Oxford, November 2012
Effect of donor age on organ retrieval in UK Organ Retrieval Workshop, Oxford, November 2012
Brain-directed therapies take precedence over systemic support Principles of brain resuscitation Therapies for the acutely injured brain • deep sedation • Intubation and controlled ventilation • maintenance of brain perfusion pressure • Osmotherapy (ICP) • Vasoconstrictors (MAP) Organ Retrieval Workshop, Oxford, November 2012
Principles of brain resuscitationICP monitoring The real complications of ICP monitoring cardiovascular collapse respiratory failure Organ Retrieval Workshop, Oxford, November 2012
Complications of ICP monitoringCardiovascular collapse The perils of maintenance of cerebral perfusion • Hypotensive sedative regimens • Osmotherapy • Hypovolaemia • Electrolyte imbalance • Vasoconstrictor therapies Organ Retrieval Workshop, Oxford, November 2012
Complications of ICP monitoringRespiratory failure The perils of denial of respiratory cares • Deep sedation and paralysis • Microaspiration • Basal atelectasis • Ventilator-acquired pneumonia • Mechanical ventilation • Bullae • Pneumothorax Organ Retrieval Workshop, Oxford, November 2012
Systemic inflammation of brain injury from Barklin, Acta Anaes Scand (2009) 53: 425-35 Human and experimental evidence for antigen-independent organ injury Organ Retrieval Workshop, Oxford, November 2012
Before and after brain death Trauma Haemorrhage / massive transfusion Aspiration Hypoxia Hospital acquired infection Mechanical ventilation Trauma and rescue therapies Organ retrieval Brain death Ischaemia / reperfusion Sympathetic storm Pulmonary capillary injury Systemic vasoconstriction and organ ischaemia Brain-derived inflammatory mediators Systemic inflammation of brain death Adapted from Barklin, Acta Anaes Scand (2009) 53: 425-35 Organ Retrieval Workshop, Oxford, November 2012
Pathophysiology of brain death Initial observations of ‘le coma dépassé’ • Haemodynamic instability • Pulmonary oedema • Hypothalamic failure • Diabetes insipidus • Poikilothermia • Disseminated intravascular coagulopathy Organ Retrieval Workshop, Oxford, November 2012
Pathophysiology of brain death Organ Retrieval Workshop, Oxford, November 2012
Pathophysiology of brain death Diabetes insipidus Organ Retrieval Workshop, Oxford, November 2012
Pathophysiology of brain death Poikilothermia Organ Retrieval Workshop, Oxford, November 2012
Pathophysiology of brain death Poikilothermia frequently overlooked vasodilatation reduced metabolic rate cool ambient surroundings may contribute to haemodynamic and haemostatic failure will continue until SVR is restored Organ Retrieval Workshop, Oxford, November 2012
Pituitary failure in brain death Diabetes insipidus • ≈ 70% incidence in BSD • Failure of neurohypophysis • Diuresis of up to 1000 ml / hr • Results in • hypovolaemia • hypokalaemia • hypernatraemia • May confound diagnosis of death and assessment of perfusion • Frequently undertreated Organ Retrieval Workshop, Oxford, November 2012
Pathophysiology of brain death Pupillary mydriasis Organ Retrieval Workshop, Oxford, November 2012
Harvey Cushing Neurosurgeon Pathophysiology of brain death Cushing’s reflex Organ Retrieval Workshop, Oxford, November 2012
Haemodynamic instability of brain death Initial observations • 80-90% of brain dead donors are haemodynamically unstable • Severity α rate of ICP rise • Frequently worse in children, young adults • Multi-factorial in its aetiology • Sympathetic storm and myocardial ischaemia • Spinal shock • Neurogenic pulmonary oedema • Diabetes insipidus • Almost always reversible, given sufficient time and effort Organ Retrieval Workshop, Oxford, November 2012
Sympathetic storm Organ Retrieval Workshop, Oxford, November 2012
Sympathetic storm Transient release of endogenous catecholamines in canine model Contraction band necrosis From Novitzky D. Selection and management of cardiac allograft donors. Current opinion in organ transplantation 1998;3:51-61. Organ Retrieval Workshop, Oxford, November 2012
Sympathetic storm ? a form of stress (Takutsubo’s) cardiomyopathy Organ Retrieval Workshop, Oxford, November 2012
Haemodynamics of brain death Regional neuraxial blockade of sympathetic storm Organ Retrieval Workshop, Oxford, November 2012
Aftermath of the sympathetic storm Persistent hypotension From Herijgers et al . The effect of brain death on cardiovascular function in rats. Part I. Is the heart damaged. Cardiovascular Research 38: 98-106 Organ Retrieval Workshop, Oxford, November 2012
Aftermath of the sympathetic storm Preserved myocardial performance in rat model of brain death Spinal shock vasoparalysis Hyperdynamic circulation From Herijgers et al . The effect of brain death on cardiovascular function in rats. Part I. Is the heart damaged. Cardiovascular Research 38: 98-106 Organ Retrieval Workshop, Oxford, November 2012
Aftermath of the sympathetic storm Preserved myocardial performance in rat model of brain death From Herijgers et al . The effect of brain death on cardiovascular function in rats. Part I. Is the heart damaged. Cardiovascular Research 38: 98-106 Organ Retrieval Workshop, Oxford, November 2012
Brain death related hypotension Organ Retrieval Workshop, Oxford, November 2012
Afterglow of one big bang Cosmic microwave background radiation Organ Retrieval Workshop, Oxford, November 2012
Afterglow of autonomic stormNeurogenic pulmonary oedema Alveolar flooding • common • frequently • misdiagnosed • mistreated • cardiogenic in origin, non-cardiogenic in behaviour • can be florid • precursor for systemic inflammatory response Organ Retrieval Workshop, Oxford, November 2012
Afterglow of autonomic stormNeurogenic pulmonary oedema Disruption of the alveolar – capillary barrier • common • frequently • misdiagnosed • mistreated • cardiogenic in origin, non-cardiogenic in behaviour • can be florid • precursor for systemic inflammatory response Organ Retrieval Workshop, Oxford, November 2012
Principles of donor management Donor management requires a fundamental shift in focus – from brain to donor organ directed therapies. Organ Retrieval Workshop, Oxford, November 2012
Catecholamines and donor therapy The case against catecholamines Catecholamines are raised during the sympathetic storm Catecholamines are implicated in contraction band necrosis Hearts from donors who have received catecholamine infusions do badly (norepinephrine) Organ Retrieval Workshop, Oxford, November 2012
Catecholamines and donor therapy The case against catecholamines Catecholamines are raised during the sympathetic storm Catecholamines are implicated in contraction band necrosis Hearts from donors who have received catecholamine infusions do badly Therefore we must not give donors catecholamine infusions Hearts may be declined when donors are on high doses of catecholamines Organ Retrieval Workshop, Oxford, November 2012
Catecholamines and donor therapy But…… outcomes in kidney transplantation • Kidneys from donors who have received catecholamine infusions do well • Cardiac injury of the sympathetic storm is reversible • Standardised donor management protocols allow retrieval of apparent unsuitable heart grafts • Restoration of normovolaemia • Correction of vasodilatation • Titrated inotropic support Organ Retrieval Workshop, Oxford, November 2012
Catecholamines and donor therapy But……. reversibility in survivors of the sympathetic storm • Kidneys from donors who have received catecholamine infusions do well • Cardiac injury of the sympathetic storm is reversible • Standardised donor management protocols allow retrieval of apparent unsuitable heart grafts • Restoration of normovolaemia • Correction of vasodilatation • Titrated inotropic support Organ Retrieval Workshop, Oxford, November 2012
Catecholamines and donor therapy But…… transformation of unacceptable donors • Kidneys from donors who have received catecholamine infusions do well • Cardiac injury of the sympathetic storm is reversible • Standardised donor management protocols allow retrieval of apparent unsuitable heart grafts • Restoration of normovolaemia • Correction of vasodilatation (vasopressin > norepinephrine) • Titrated inotropic support (dopamine > epinephrine) Wheeldon et al. Transforming the unacceptable donor. J Heart Lung Transplant. 1995; 14: 734-742 Organ Retrieval Workshop, Oxford, November 2012
Hormone replacement therapy The case for hormone replacement Organ Retrieval Workshop, Oxford, November 2012
Donor optimisationEarly observations • Hypotension is bad for kidneys • Catecholeamines may be bad for hearts…….. • …….. but good for kidneys • Hormone replacement may be good for hearts • Invasive haemodynamic monitoring may be good for thoracic organs…………if you know how to use it • Some ICU clinicians seem reluctant to deliver it Critical care of the potential organ donor is not a passive process and should start as early as possible. Organ Retrieval Workshop, Oxford, November 2012
Donor Care Bundle Organ Retrieval Workshop, Oxford, November 2012
Donor care bundleKey initial priorities • Assess fluid status and correct hypovolaemia • Introduce vasopressin infusion and where required introduce flow monitoring • Perform lung recruitment manoeuvres (e.g. following apnoea tests, disconnections, deterioration in oxygenation or suctioning) • Identify, arrest and reverse effects of diabetes insipidus • Administer methylprednisolone (all donors) Organ Retrieval Workshop, Oxford, November 2012