Download
1 / 16
160 likes | 244 Views
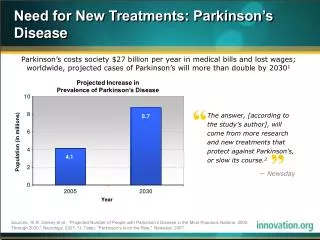
Keeping patients with Parkinson’s ‘switched on’. Parkinson’s Disease. A progressive neurological condition. Affects around 120,000 people in the UK.

E N D
Parkinson’s Disease • A progressive neurological condition. • Affects around 120,000 people in the UK. • Caused by a loss of nerve cells in the substantia nigra in the brain which produce dopamine. About 80% of nerve cells in this area are lost before symptoms appear. • Cause = unknown ? Genetics, ?environmental • Dopamine helps control and coordinate body movements3 main symptoms: • Bradykinesia and lack of coordination • Tremor • Muscle rigidity
Management Medications cannot prevent disease progression but can improve quality of life. • Levodopa: amino acid precursor of dopamine. Absorbed by nerve cells in the brain and turned into dopamine. • Dopamine agonists: act as a substitute for dopamine. • Monoamine Oxidase-B Inhibitors: block monoamine oxidase-B which destroys dopamine. • Catechol-O-Methyltransferase Inhibitors: prevent peripheral breakdown of levodopa by inhibiting the enzyme COMT, allowing more levodopa to reach the brain.
Medication Timings and Omissions Every person with Parkinson’s has a different experience of the condition and is affected by symptoms to a varying extent and at different times. Therefore, medication regimes are developed with a specialist and tailored to the individuals needs. (Parkinson’s UK 2010).
NICE guidelines (2006) • “Antiparkinsonian medication should not be withdrawn abruptly to avoid the potential for acute akinesia or neuroleptic malignant syndrome.” • “In view of the risks of sudden changes in antiparkinsonian medication, people with PD who are admitted to hospital or care homes should have their medication: • given at the appropriate times, which in some cases may mean allowing self-medication. • adjusted by, or adjusted only after discussion with, a specialist in the management of PD.”
“dyskinesia” “rigidity” “hallucinations” “switched off” “swallowing difficulties”“anxiety” “freezing” “loss of confidence” “confused” “can’t move” “depression” “constipation”“apathy” “can’t sleep” “cognitive problems”
If an individual omits to take their medication, or does not take it on time, then their medication levels will be low and they may experience an ‘off’ period. This may involve worsened motor symptoms e.g. be unable to move, disturbed bowel and kidney function, mood and sleep disruptions, hallucinations (Parkinson’s UK 2011).
The knock on effect... • Patients with PD have longer stays in hospitals (2-14 days longer) than patients without PD (Gerlach et al 2011, Aminoff et al 2011). • Delayed rehabilitation e.g. unable to participate in physiotherapy (Elphick et al 2006a). • Nutritional problems e.g. unable to swallow resulting in weight loss (Elphick et al 2006a). • Decreased quality of life for the individual, their carer and their family. • Increased costs to the NHS.
Therefore, adhering to an individuals medication regime is very important to achieve optimal symptom control.
However... US study of hospital records: 3873 doses of PD medications prescribed. 675 incorrect medication administrations. Of which, 322 were omitted, 300 late by ≥ 30 mins, 53 early by ≥ 30 mins. Contraindicated medications prescribed for 19 patients (Hou et al 2012). UK study of case notes and drug cards: 73 out of 104 (70%) patients with PD experienced a delay in receiving their first dose of PD medication. 81% of these patients experienced at least one dose omission. Average of 8.2 dose omissions per patient (Elphick et al 2006b). In a UK hospital, only 6 out of 104 PD patients self medicated during admission (Elphick et al 2006b) .
Even more importantly, the patient and carer perspective... “nobody listens, you try and tell them something and they think they know better all the time...if you are taking them everyday, you know when you need to take them; your body tells you” (Inpatient with PD). Buetow et al 2010
"Each fresh ward sister bustled suspiciously up to my husband demanding to know why he was medicating himself, what drugs he was taking and when. We must have given them the list half a dozen times ... their attitude was certainly not accommodating” (wife of patient with PD). Parkinson’s UK 2006
“They (hospital staff) do not always understand the way the PD medications work...were not aware, I think, of the need for Parkinson’s people to have their medication at a given time” (Inpatient with PD). “They regard the time as a suggestion...an indication of when you might get them” (Inpatient with PD). Buetow et al 2010 http://www.parkinsons.org.uk/advice/publications/professionals/get_it_on_time_hospital_dvd/video_get_it_on_time_hospital.aspx
What nurses can do... • Educate themselves and be aware of the importance of adhering to individual’s Parkinson’s medication regimes. • Listen to patients and their carers and work with them and the multidisciplinary team to make sure we get it right (Buetow et al 2010). • Make referrals to specialists where required. Hou et al (2012) – correct medication administration was significantly higher in PD patients who had neurological consultations compared to those who did not. • Assess and allow self medication where appropriate.
References Aminoff, M.J., Christine, C.W., Friedman, J.H., Chou, K.L., Lyons, K.E., Pahwa, R., Bloem, B.R., Parashos, S.A., Price, C.C., Malaty, I.A., Iansek, R., Bodis-Wollner, I., Suchowersky, O., Oertel, W.H., Zamudio, J., Oberdorf, J., Schmidt, P. and Okun, M.S.(2010) ‘Management of the hospitalized patient with Parkinson’s Disease: Current state if the field and need for guidelines’, Parkinsonism and Related Disorders, 17, pp 139-145. Buetow, S., Henshaw, J., Bryant, L. and O’Sullivan, D. (2010) ‘Medication timing errors for Parkinson’s Disease: Perspectives held by caregivers and people with Parkinson’s in New Zealand’, Parkinson’s Disease, pp 1-6. Elphick, H., Bolam, D. and Liddle, B. (2006a) ‘Managing Parkinson’s Disease medication in hospital: The patient’s perspective’, Age and Ageing, 35 (1), p i64. Elphick, H., Madan, S. and Liddle, B. (2006b) ‘Provision of Parkinson’s Disease medication to hospital inpatients’, Age and Ageing, 35 (1), p i63.
Gerlach, O., Winogrodzka, A. and Weber, W. (2011) ‘Clinical problems in the hospitalized Parkinson’s Disease patient: Systematic review’, Movement Disorders, 26 (2), pp 197-208. Hou, J.G., Wu, L.J., Moore, S., Ward, C., York, M., Atassi, F., Fincher, L., Nelson, N., Sarwar, A. and Lai, E.C. (2012) ‘Assessment of appropriate medication administration for hospitalized patients with Parkinson’s Disease’, Parkinsonism and Related Disorders, 18, pp 377-381. NICE (2006) Parkinson's disease: Diagnosis and management in primary and secondary care. London. Parkinson’s UK (2011) Living with Parkinson’s, London. Parkinson’s UK (2010) Drug treatments for Parkinson’s, London. Parkinson’s UK (2006) ‘Get it on time’ campaign, Available at: www.parkinsons.org.uk/about_us/policy_and_campaigns-1/campaigns/get_it_on_time_campaign/campaign_background.aspx (Accessed 7 May 2012).