Download
1 / 3
30 likes | 162 Views
Introduction. Results. Method. Conclusions. The Self versus Others Distinction in Inflated Responsibility for Harm: Implications for the Cognitive Model of OCD. Jesse R. Cougle, Han-Joo Lee, Michael J. Telch. The University of Texas at Austin, Laboratory for the Study of Anxiety Disorders.

E N D
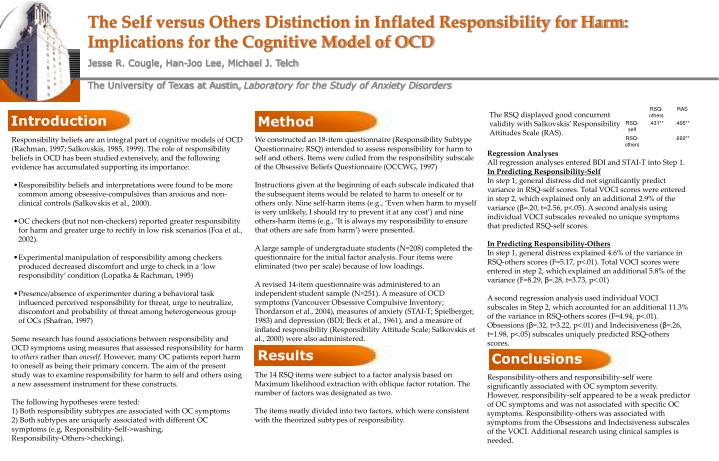
Introduction Results Method Conclusions The Self versus Others Distinction in Inflated Responsibility for Harm: Implications for the Cognitive Model of OCD Jesse R. Cougle, Han-Joo Lee, Michael J. Telch The University of Texas at Austin, Laboratory for the Study of Anxiety Disorders Regression Analyses All regression analyses entered BDI and STAI-T into Step 1. In Predicting Responsibility-Self In step 1, general distress did not significantly predict variance in RSQ-self scores. Total VOCI scores were entered in step 2, which explained only an additional 2.9% of the variance (β=.20, t=2.56, p<.05). A second analysis using individual VOCI subscales revealed no unique symptoms that predicted RSQ-self scores. In Predicting Responsibility-Others In step 1, general distress explained 4.6% of the variance in RSQ-others scores (F=5.17, p<.01). Total VOCI scores were entered in step 2, which explained an additional 5.8% of the variance (F=8.29, β=.28, t=3.73, p<.01) A second regression analysis used individual VOCI subscales in Step 2, which accounted for an additional 11.3% of the variance in RSQ-others scores (F=4.94, p<.01). Obsessions (β=.32, t=3.22, p<.01) and Indecisiveness (β=.26, t=1.98, p<.05) subscales uniquely predicted RSQ-others scores. Responsibility-others and responsibility-self were significantly associated with OC symptom severity. However, responsibility-self appeared to be a weak predictor of OC symptoms and was not associated with specific OC symptoms. Responsibility-others was associated with symptoms from the Obsessions and Indecisiveness subscales of the VOCI. Additional research using clinical samples is needed. The RSQ displayed good concurrent validity with Salkovskis’ Responsibility Attitudes Scale (RAS). • We constructed an 18-item questionnaire (Responsibility Subtype Questionnaire; RSQ) intended to assess responsibility for harm to self and others. Items were culled from the responsibility subscale of the Obsessive Beliefs Questionnaire (OCCWG, 1997) • Instructions given at the beginning of each subscale indicated that the subsequent items would be related to harm to oneself or to others only. Nine self-harm items (e.g., ‘Even when harm to myself is very unlikely, I should try to prevent it at any cost’) and nine others-harm items (e.g., ‘It is always my responsibility to ensure that others are safe from harm’) were presented. • A large sample of undergraduate students (N=208) completed the questionnaire for the initial factor analysis. Four items were eliminated (two per scale) because of low loadings. • A revised 14-item questionnaire was administered to an independent student sample (N=251). A measure of OCD symptoms (Vancouver Obsessive Compulsive Inventory; Thordarson et al., 2004), measures of anxiety (STAI-T; Spielberger, 1983) and depression (BDI; Beck et al., 1961), and a measure of inflated responsibility (Responsibility Attitude Scale; Salkovskis et al., 2000) were also administered. • The 14 RSQ items were subject to a factor analysis based on Maximum likelihood extraction with oblique factor rotation. The number of factors was designated as two. • The items neatly divided into two factors, which were consistent with the theorized subtypes of responsibility. • Responsibility beliefs are an integral part of cognitive models of OCD (Rachman, 1997; Salkovskis, 1985, 1999). The role of responsibility beliefs in OCD has been studied extensively, and the following evidence has accumulated supporting its importance: • Responsibility beliefs and interpretations were found to be more common among obsessive-compulsives than anxious and non-clinical controls (Salkovskis et al., 2000). • OC checkers (but not non-checkers) reported greater responsibility for harm and greater urge to rectify in low risk scenarios (Foa et al., 2002). • Experimental manipulation of responsibility among checkers produced decreased discomfort and urge to check in a ‘low responsibility’ condition (Lopatka & Rachman, 1995) • Presence/absence of experimenter during a behavioral task influenced perceived responsibility for threat, urge to neutralize, discomfort and probability of threat among heterogeneous group of OCs (Shafran, 1997) • Some research has found associations between responsibility and OCD symptoms using measures that assessed responsibility for harm to others rather than oneself. However, many OC patients report harm to oneself as being their primary concern. The aim of the present study was to examine responsibility for harm to self and others using a new assessment instrument for these constructs. • The following hypotheses were tested: • 1) Both responsibility subtypes are associated with OC symptoms • 2) Both subtypes are uniquely associated with different OC symptoms (e.g, Responsibility-Self->washing, • Responsibility-Others->checking).
Introduction Results Period 1 Think anything and record ANX manipulation ANX manipulation No ANX manipulation No ANX manipulation Think anything record Suppress record Think anything record Suppress record Period 2 Think anything and record Period 3 Conclusions Method The Singular and Combined Effects of Thought Suppression and Anxiety Induction on Frequency of Threatening Thoughts: An Experimental Investigation Jesse R. Couglea, Mark B. Powersa, Han-Joo Leea, Jasper A.J. Smitsb, Richard Seima, Michael J. Telcha aThe University of Texas at Austin, Laboratory for the Study of Anxiety Disorders bSouthern Methodist University, Department of Psychology • Because Period 2 thought frequency was associated with Period 1 state anxiety, r =.31, p<.001, suppression effort, r=.30, p<.001, and thought frequency, r=.61, p<.0001, these Period 1 variables were included as covariates in the analyses. Under conditions of heightened anxiety, a ‘reverse rebound’ effect was found, with participants in the suppression condition reporting significantly fewer thoughts in Period 3 than participants in the no suppression condition. This finding was not observed for participants in the no anxiety condition. Under conditions of heightened anxiety, participants who suppressed reported a significantly lower percentage of time spent thinking about their target thoughts than participants who did not suppress. This was found for Periods 2 and 3. No effects of suppression were found in the no anxiety condition. No paradoxical effects of thought suppression were found for target thought discomfort. • Thought suppression was more successful under conditions of heightened anxiety. • Anxiety does not appear to act as a cognitive load when suppressing anxious thoughts. Research into the paradoxical effects of thought suppression has its beginnings in Wegner and colleagues’(1987) famous ‘white bear’ experiment. In this study, participants who were asked to suppress thoughts of a white bear subsequently reported a greater frequency of white bear thoughts compared to those who had not been instructed to suppress. Since Wegner’s study, the effects of thought suppression have been studied extensively, and thought suppression has been given a prominent role in cognitive models of OCD (Salkovskis, 1999) and PTSD (Ehlers & Clark, 1999). According to Wegner (1994), situations involving cognitive load (e.g., rehearsing a 9-digit number) lead to enhanced paradoxical effects of suppression. This may have special clinical significance when applied to the study of anxiety disorders. Anxiety has been conceptualized as a type of cognitive load that affects working memory capacity (Sorg & Whitney, 1992). Suppression of intrusive thoughts is common among obsessive-compulsives and PTSD sufferers, and suppression often occurs for these individuals when they are in an anxious state. If anxiety functions as a cognitive load similar to time constraint and number rehearsing, then suppression under anxiety-provoking conditions should have counterproductive effects. The central aim of the present study was to investigate the singular and combined effects of thought suppression and anxiety induction on the frequency and duration of personally relevant thoughts of a threatening nature. To insure that our anxiety manipulation (anticipated impromptu speech) would elicit sufficient anxiety, we specifically selected participants scoring high on social anxiety. We predicted that participants given suppression instructions under conditions of heightened anxiety would report a greater frequency and duration of target thoughts during the suppression and post-suppression periods. • Sample: 138 UT undergraduates displaying high social anxiety participated on the experiment. All participants scored at the 75th percentile or above on the Leibowitz Social Anxiety Scale (LSAS; Leibowitz, 1987) • Procedure: Participants first completed a questionnaire battery. The target thought used during the thought monitoring intervals was taken from their responses on the Assessment of Social Concerns (ASC; Telch et al., 2004). A standard thought suppression design was used with the addition of an anticipated speech anxiety manipulation (see Figure 1). The anxiety induction consisted of instructions that lead participants to believe that they would have to give a 3-min. impromptu speech. • A 2 X 2 X 2 repeated measures ANCOVA was performed on target thought frequency and duration. • Within-subjects factor: Assessment Period (Time 2 vs. Time 3) • Between-subjects factors: Suppression condition (suppress vs. no suppress) and Anxiety condition (ANX vs. CTRL)
Introduction Results Conclusions Method Placebo Controlled Trial Investigating the Efficacy of Encouraging Anti-Phobic Actions during In Vivo Exposure Therapy: Work in Progress Kate B. Wolitzky & Michael J. Telch University of Texas at Austin Measures: Outcome: Acrophobia Questionnaire (AQ) Behavioral Approach Test-1 (BAT-1) outside parking garage Behavioral Approach Test (BAT-2) inside stairwell Heart rate and SUDS ratings during BATs Maintaining Factors: Safety Behavior Checklist for Acrophobia (SBCA) Procedure: Pre-treatment assessment included a CIDI diagnosis of Specific Phobia, Natural Environment Type (Acrophobia), and 2 BATs (above). Eligible participants returned the following week and were randomly assigned to one of three treatment conditions, each lasting one hour, consisting of six, 6-minute trials. The three conditions were: Exposure with anti-phobic actions Exposure only Credible placebo control (Digital Audio Visual Integration Device, DAVID) After treatment, participants returned one week later to complete a post-treatment assessment (similar to pre-treatment assessment) and a one-month follow-up assessment. Exposure is known to be highly effective in treating specific phobias. However, exposure does not work for all patients, and some show a return of fear at follow-up assessments. Thus, examining the mechanisms that drive fear reduction during exposure can help researchers develop more potent treatments, while also shedding light on the nature of anxiety disorders. Research in our laboratory (Sloan & Telch, 2000; Powers et al., 2004) and in the UK (Salkovskis et al, 1991; Wells et al., 1995) suggests that patients who rely on safety aids and defensive behaviors while confronting their phobic threats display poorer treatment outcome than patients who do not use safety aids or who use them initially but fade them during treatment. Moreover, it appears that the mere perceived availability of safety aids – even when they are not actually utilized also undermines the efficacy of exposure treatments (Powers et al., 2004). We reasoned that if the presence of safety aids and the engagement in safety behaviors during treatment undermines exposure treatment outcome, perhaps the introduction of actions incompatible with these defensive behaviors would actually facilitate the effects of exposure. We refer to these actions as “Anti-Phobic” strategies. Examples include holding one’s hands behind one’s back as opposed to holding on to the rail of a balcony for a height phobic, or running towards the balcony railing as opposed to backing away from it. Telch (2004) has provided anecdotal support for the value of adding these anti phobic strategies to traditional exposure therapy. The present study, which is still in progress, attempts to provide a stringent test of the incremental utility of incorporating anti-phobic strategies during exposure therapy for acrophobia. Univariate ANCOVAs controlling for pre-treatment scores were conducted. All three conditions significantly improved on all outcome measures. Significant group differences were observed on BAT-1 post peak fear (F = 8.92, p < 0.001) and post BAT-2 fear (F = 8.16, p < .001). Bonferroni post-hoc tests revealed that the exposure with anti-phobic actions group reported significantly lower fear on the BATs than the other 2 groups. • At posttreatment, participants receiving exposure with anti-phobic actions significantly outperformed those receiving either exposure alone or a placebo control. • The superiority of exposure with anti-phobic actions was seen on multiple indices of height-related fear at posttreatment. • Although follow-up data are not yet complete, preliminary findings suggest that participants receiving pulsed audio-video stimulation at a frequency of 8 hz displayed additional gains during the follow-up period, which were not observed for the two exposure conditions. • These preliminary data suggest that encouraging phobic individuals to engage in anti-phobic actions while confronting their phobic threat may enhance treatment outcome at least in the short-term. Moderate to large effect sizes were observed for the comparisons between exposure with anti-phobic actions and exposure only i.e., AQ post (d = 0.64), AQ f/u (d = 0.74), SCBA post (d = 0.61), BAT-1 fear post (d = 1.15), BAT-2 fear post (d = 1.68), and BAT-2 fear f/u (d = 1.48). Moderate to large effect sizes were also observed for the comparison of exposure with anti-phobic actions and our credible placebo control (audio-visual photic stimulation) i.e., SBCA post (d = 0.81), BAT-1 fear post (d = 1.43), and BAT-2 fear post (d = 1.31). Participants: Participants (N = 43) displaying a marked fear of heights and meeting DSM-IV criteria for specific phobia were recruited through the Austin community and Introductory Psychology classes. The final sample was predominantly female (70%) and Caucasian (58%). Ten participants are still waiting to complete their one-month follow-up assessments.