Download
1 / 135
1.36k likes | 1.57k Views
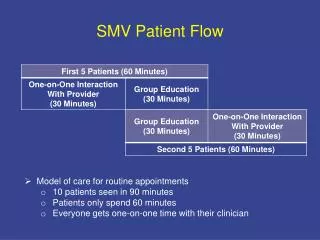
Patient Flow Collaborative. Angela Peluso - Clinical Lead Ian Jackson - Presenter Eastern Health – Maroondah Hospital. Summarise Organisational Constraint areas. Bed Management - Admission delays for elective surgery - Admission delays from ED Acute/Sub Acute

E N D
Patient Flow Collaborative Angela Peluso - Clinical Lead Ian Jackson - PresenterEastern Health – Maroondah Hospital
Summarise Organisational Constraint areas • Bed Management - Admission delays for elective surgery - Admission delays from ED • Acute/Sub Acute - Delayed access to Rehab & NH beds • Theatre Utilization - High HIP rate
Summarise Priority Constraint Area 2 • Acute to Sub Acute -Delayed access to NH Beds -Delayed access to Rehab beds
Diagnostic work • Ward sample data repeated -Confirmed previously identified constraints • Brainstorming session -Included all stakeholders – NUM’s, Allied Health, Medical Rep (Geriatrician), Reps from off-site rehab facilities -Confirmed process issues and recommended these be mapped • Process Mapping session -Identified key constraints in transition process
Diagnostic work cont. • Staff reactions -Committed to “doing something” to improve things - Enthusiastic about possibilities - Acknowledgement that even small changes could have big effects - “Lets do it!”
Improvement Plan • Establish clinical area team - Identify clinical area team leader - Include key stakeholders -Medical representative – Geriatrician - Rep from PJC - NUM’s from GEM, ortho & medical wards - Allied health – social worker & physio - Aged care nurse consultant
Improvement Plan Cont. • Investigate the following six key areas identified as contributing to delays • Referral process to allied health • Organising OT home visits • ACAS referral process • Refusal of rehab bed by patient/family • Delays in discharge summary documentation • Out of hours communication with central booking office
Progress Implementing the following changes • Faxing allied health referrals • NUM generated ACAS referrals • Improved communication channels with centralized bookings office
Lessons learnt • Need for all key stake holders to be involved -delivers better more sustainable outcomes • Select “right person” for “right job” -need to be motivated & outcome focused • “Rome wasn’t built in a day” -be patient
Desired Impact • Reduce LOS • Reduce 12 hour waits in Ed • Better more effective communication channels between sites • Improved patient care
Next Steps • Review and update relevant policies & procedures • Review admission/discharge criteria for hospital GEM ward
Patient Flow Collaborative Janine Rogers, CHIP Manager Calvary Health Care ACT
Summarise Organisational Constraint areas • Allied Health (AH) referral process- inappropriate & not timely • Radiology-timeliness & accessibility • Nursing Paperwork-duplicative & excessive • VMO Rounds-disjointed & not well managed from • ACAT Services-limited appointments & difficulties with rebooking
Summarise Priority Constraint Area 1 • AH Issues • Inappropriateness of referral • Timeliness of referral • Referral process
Diagnostic work • Brainstorming • Ad hoc referral arrangements • Timing issues • Communication issues • Consumer • Not seen in ED • Determine what is process now • Tick and flick exercise in ED and Medical for • Response times • Relevance of referral • Who is making referral • Process effectiveness.
Improvement Plan • AH referral indicators • Determine indicators • Pilot in two areas, then • Specific to each service area • Refine process • Determine time intervals from referral to assessment and then set optimum goal • Structured flow for referral • Facilitate communication between parties • Streamline process • Ease of access to contact # and names
Progress • AH referral audit underway • Referral process set into flow diagram • Specific AH Indicators for pilot accepted • AH and nursing input • Evaluation audit on pilot to be completed
Lessons learnt • Managing detractors and concerned staff • Getting everyone in the right place at the right time • Reliance on senior 3rd party to share project information • Don’t do this during accreditation
Desired Impact • Timeliness • Patients requiring AH intervention to be seen within …?…. (optimal time frame) • Appropriateness • All AH referrals to have a clear rationale for assessment • Knowledge • Increase knowledge across hospital on referral indicators • Communication • % of referrals that follow correct communication process
Next Steps • Radiology mapping • Revise nursing assessment • Standardise across hospital • Standardise risk assessments • Include expectation management • Increase efficiency of VMO rounds • ACAT service
Team Presentations Melanie Hendrata and Kim Moyes 5TH October 2004
Concurrent Session 1Team Presentations Bellarine Room 3 • Northeast Health - Wangaratta • Bendigo Healthcare Group • Southern Health – Dandenong Hospital • Peninsula Health • Box Hill Hospital
Patient Flow Collaborative Christine Giles Northeast Health Wangaratta
Rigorous Diagnostics • Poor communication pathways both verbal and written- Inadequate or incorrect documentation of patients’ social & medical history. • Inconsistencies with quality of admission data from GP’s and referring agencies.
Rigorous Diagnostics • Patients being asked the same questions repeatedly by different personnel. • Organisation duplication of paperwork. • Discharge dependant on timing of medical rounds, availability of bed elsewhere, family. • Delays in radiology.
Organisational Constraint Areas • Communication and Information Transfer. • Emergency Department-time taken between decision to admit and admission to ward. • Medical ward LOS-activities affecting discharge, transfer & readmissions.
Implementation Phase- Plan, do, study, act. • Team members further brainstormed the constraint areas. • Communication between ED and Medical unit • INR monitoring and warfarin therapy • Nurse initiated clinical guidelines • Discharge-time and trends in the Medical unit • Quality of admission data • Delays in ED-causes and effect • Form review by Medical Records. • Consensus reached on plan, do, study act initiatives.
Implementation Phase-Diagnostic work Tools Desk top audits, tally sheets, staff interviews both structured and unstructured, questionnaires, existing hospital data. Who was involved? Health information manager, ED, medical unit, nursing staff and clerical staff, ward nurses, executive, junior and senior medical staff, director of pharmacy, director of radiology, under graduate student. Patients and relatives.
Implementation Phase-Diagnostic work What data/information was really useful/not useful? Anecdotal, face to face staff interviews, audits, previous studies, patient comments. 1. Face to FaceRadiology delays as an issue debunked. New filmless system being implemented. Delays in the request for and actioning pathology results highlighted- INR-therapeutic range and warfarin dose. 2. INR Clinical Indicator Variance Analysis 2003 This data supports anticoagulation management as one of our perceived causes of medical ward prolonged LOS affecting discharge, transfer & readmission.
Implementation Phase-Diagnostic work 3. Desktop audit indicated excellent compliance by NHW with discharge summaries but raised some questions about the quality of information accompanying patients on arrival to our hospital. Identified some evidence of GP admitted patients having increased LOS for certain patient types. 4. Tally sheets!!-poor compliance, hostility, paperwork fatigue led to insufficient data.
Implementation Phase-Diagnostic work Staff reactions- • Anger. • Disinterest. • Passive resistance. • Frustration. • Ability to see what needs to be done but negative about means to achieve change. • Powerlessness. • Blame culture.
Improvement and Progress • Medical ward and ED identified as the most pressing communication issue. Positive channels of communication to be established and shared goals initiated • Reduce duplication in history taking, trial innovations to ease the burden of the admission to ward process. • Explore MAPU to improve patient flow. • Established a forum for both groups to have dialogue and understand each other’s issues.
Improvement and Progress 2. Communication with Medical staff group to establish key responsibilities for investigating identified constraints • Engage GPs-review admission process, LOS. • Exploration of nurse initiated activities to expedite the discharge/transfer process i.e.pathology requests, referrals to allied health, medication. • Identification of the use of evidence based care, clinical practice guidelines, beginning with anti-coagulation therapy.
Lessons learnt • Separate fact from opinion. • Distil the problem from the symptoms. • Examine data quality carefully and adapt diagnostic tools to be contextually appropriate- “you can’t weigh something with a tape measure” • Accept that change is painful but good leadership can transform negative energy into a positive outcome. • Harness the energy of the organisation champions.
Next Steps • Trial MAPU. • Develop education plan for Medical ward and ED nursing staff re history taking, referral, pathology and pharmaceuticals skills. • Develop an education plan for admission clerical staff and external referral agencies re accuracy of patient information. 4. Engage junior medical staff in a culture of teamwork and evidence based practice, clinical practice guidelines.
Patient Flow Collaborative June DysonBendigo Health Care Group
BHCG Organisational Constraint areas • Variation in patient management practices by doctors and nursing staff for Stroke patients. Impacts on quality of care and length of stay • Limited availability of acute, rehab and aged care beds
BHCG Organisational Constraint areas • Availability of registrars to assess potential admissions in the Emergency Department (ED) • Repetitive documentation, assessment and data capture for patients
Priority Constraint Variation in patient management for Stroke • Stroke is a discrete and important area across the continuum. • There is some evidence that: • Stroke care and treatment could be improved in the ED • Stroke care and treatment could be improved in the acute phase • Stroke patients spend time additional time in acute beds when they are ready for discharge • Follow-up for TIA and Stroke patients in the community could be improved.
Diagnostic work • Stroke patient journey times • A data collection tool was developed to better understand the timing of the patient journey. • Developed by the Executive team in collaboration with ED, acute and rehab staff. • Difficulty in reaching consensus on tool - the tool was drafted at least six times. • Consumers were not involved at this point. • The data collection is in progress (it took six weeks to reach agreement on the tool and manner of data collection)
Diagnostic work • Stroke residential care patients • A SPC analysis of stroke length of stay (2001-004) identified a number of ‘special causes’ • We reviewed the patient histories of ‘special causes’ to determine the reasons for long lengths of stay • Particularly we looked at the time frames between acute admission, Aged Care Assessment team assessment, placement on residential care waiting list • This was compared to existing data looking at Stroke referral time to rehabilitation and residential care.
Diagnostic work: Long LOS • The data was consistent with staff’s beliefs about the difficulty in finding residential care placements. • A small subset of cases for Stroke LOS identified data collection problems • There is a ‘weariness’ about the difficulties in finding residential care placement. It is ‘out of our hands’. • The data did not provide clues to how to improve patient flow.