Download
1 / 50
520 likes | 1.5k Views
Initial Presentation. 31 y/o G5P2022 EDC 9/10/03, LMP 12/7/02

E N D
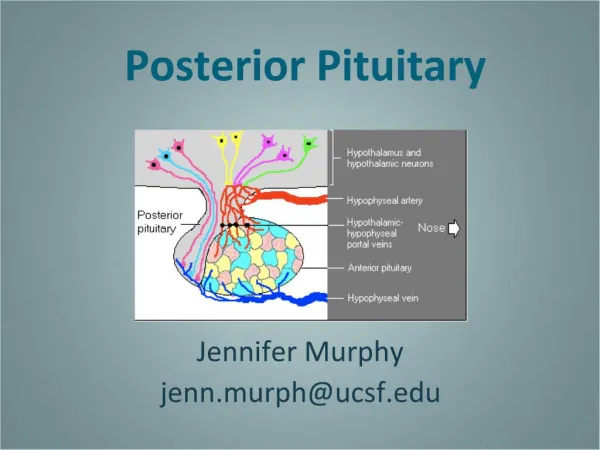
1. Posterior Urethral Valve Syndrome Dr. Tricia A. Jacobsen
6/30/03
2. Initial Presentation 31 y/o G5P2022
EDC 9/10/03, LMP 12/7/02 � conceived on OCP�s
Preg dated by LMP, conf by 7W1D u/s
Prenatal course uncomplicated prior to admission
3. Past OB Hx 2 Spontaneous Abortions
2 Spontaneous Vaginal Deliveries - uncomplicated
4. Past GYN Hx No h/o of ovarian disease
No abnormal Pap Smears
No h/o STD�s
Menses regular, began at age 12
5. Past Surgical Hx No surgical history
6. Past Medical Hx H/O Migraines
Meds � Lo-estrin 1/20 with Fe
NKDA
Social � � PPD cig.
Occ ETOH
7. Prenatal labs O+, Antibody screen neg
RI, VDRL NR
Hep B Sag � neg
HIV neg
CBC � 6.8/13/36.7/304
Pap � WNL
One hour Glucola � 52
Quad Screen � DS risk neg; 1:622
8. 16 week u/s � 4/2/03 Anatomy Scan � wnl
Amniotic fluid � Volume wnl
Normal IUP est. at 16w5d consistent with LMP
EFW of 159 grams
Placenta � fundal, no evidence of previa
9. 6/17/03 Called Attending MD c/o contractions
c/o mild contractions or �Cramping�
No LOF, No Vaginal bleeding
Positive Fetal Movement
Prenatal course uncomplicated until that day
No other illnesses or symptoms
10. 6/17/03 cont. Pt sent for an ultrasound in Rocky Hill
Found to have oligohydramnios with a 3 cm pocket
Distended fetal bladder 4.9 cm by 2.9 cm
Bilateral hydronephosis
Pt sent to Labor and Delivery for complete evaluation
11. Evalulation on L&D � 6/17/03 PE - no acute distress, no h/a, scotomata
- VS: 122/72, 84, 98.7
Lungs �CTA, no wheezing
CV � RRR, S1S2
Abd � Soft, NT, +BS, no RUQ pain, + FM
Ex � NT, no edema
Spec � os appeared closed, Cultures sent, Nitrazine neg, fern neg, no pooling
Pelvic � Cx long, thick, closed
FHR � 130�s, reactive, Ave LTV, no variable, no decels
Toco � negative � occasional cramp
12. Evaluation on L&D - 6/17/03 cont. Labs � O+, Antibody screen neg
CBC � 8.8/12.2/34.0/252 Chem 7 � WNL
U/A � WNL
GC/CHL � neg/neg
GBS - neg
13. 6/17/03 eval cont. U/S revealed 27 wk fetus in cephalic presentation, AFI < 3 cm, + FM, FB, Placenta anterior, Grade 1
Distended bladder noted, + hydronephrosis
Pt admitted, Celestone started, MFM consulted and formal u/s ordered for the am
Pt remained on L&D for continuous monitoring due to oligohydramnios
14. MFM Evaluation began 6/18/03 � formal ultrasound revealed
Distended, thick walled bladder with a keyhole appearance in the area of the posterior urethra
Ureters and renal calyces were distended
Hydronephrosis � Left renal pelvis = 7 mm
Right renal pelvis = 10 mm
-- Amnioinfusion with 300 cc of warm normal saline was performed with asp. of 20 cc for chromosomal analysis
16. MFM Eval. Cont. Chromosomal (FISH) Analysis:
Chrom #13 = 2
Chrom #18 = 2
Chrom #21 = 2
Chrom X = 1
Chrom Y = 1
Normal Male Fetus
17. Posterior Urethral Valve Syndrome Bladder outlet obstruction that is produced by a membrane within the posterior urethra
Within the scope of obstructive uropathies
Urethral atresia
Persistent cloaca
Chromosomal abnormalities
Hypospadius, epispadius or stenosis
18. PUVS Cont. Incidence = 1 in 5,000 to 8,000 males
Affects only males
Most common cause of severe obstructive uropathies
Etiology � may be failure of complete disintegration of the urogenital membrane
19. PUVS - Diagnosis Distended, thick walled bladder with a dilated posterior urethra � �Keyhole� app.
Dilated ureters with b/l hydronephrosis
Fluid volume/urine volume varies
Presence of increased cortical echogenicity w/ or w/o cortical cysts may be consistent with renal dysplasia and a poor prognosis
Cortical cysts are associated with irreverisble, advanced renal damage � fetus not amenable to intervention
20. Classic �Keyhole� Sign
21. Rt Kidney
22. Thickened bladder wall
23. Left Kidney
24. Distended Bladder
25. Dilated Rt and Lf Ureters
26. Dilated Right Kidney
27. Left Kidney
28. Left Kidney
29. Right Kidney
30. PUVS - Pathology Obstruction appear to be a diaphragmatic membrane with small opening in posterior urethra
Simple mucosal membrane with fibrous stroma
Dilatation of the prostatic urethra occurs b/w the obstructing membrane and the bladder neck
31. PUVS - Findings Elevated intravesicular pressures leading to reflux to ureters and renal pelvises
Hydronephrosis develops from continued urine production with obstruction
Renal pelvis and calyceal systems become distended, compress renal parenchyma
32. PUVS - Findings Histologically � Smooth muscle hypertrophy and hyperplasia within the bladder wall � increased bundle of smooth muscle
Dilation of distal and proximal tubules associated with peritubular and interstitial fibrosis
Fibrosis = echogenic appearance of the renal parenchyma on ultrasound
33. PUVS After 14 wks, amniotic fluid is dependent on fetal urine production
Fetal swallowing, breathing, and AFI falls dramatically
During 18 � 24 week from canalicular to alveolar phase results in underdeveloped lungs if no fluid
34. Work up � First step � ultrasound Bladder evaluated prior to and following drainage by fine needle vesicocentesis
Overall size of bladder and degree of proximal urethral dilation (keyhole sign)
Urethral and kidney evaluation for dilation or abnormalities, echogenicity, or cysts
After vesicocentesis � the degree of bladder thickness is assessed
Rule out other anomalies ie NTD, cardiac defects
35. WU � ultrasound cont Long axis of the kidney is measured when evaluating underlying hydronephrosis
Kidneys which are large for gestational age and are less hyperechogenic � better prognosis
Kidneys which are hyperechogenic and are small have poorer prognosis due to advanced renal fibrosis
36. Work up � Second step Prenatal evaluation for fetal karyotype
Amniocentesis if fluid available � fluid may be infused the aspirated to obtain cells
CVS if early � prelim results in 2-3 days
Final results in 7-10 days
May cultures cells from fetal urine � although more difficult to culture
37. Final Eval � Third step Evaluation of fetal kidney function with sequential vesicocenteses
Completely drain fetal bladder at 48-72 hr intervals at a minimum of three occasions
Fetuses w/ progressive hypotonicity and values that fall below threshold benefit from in utero intervention i.e. shunt placement
38. Needle Aspiration of Bladder
39. Eval cont Fetuses with isolated megacystis, bilateral hydronephrosis, decreased amniotic fluid volume, absent anomalies, a 46 XY karyotype and serially improving hypotonicity with values below the recommended thresholds would be candidates for vesicoamniotic shunt placement
40. Prognosis Outcome depends upon severity
Classified as good or poor
Poor prognostic factors include diagnosis before 24 wks, oligohydramnios, increased cortical echogenicity with cysts indicating renal dysplasia and marked hydronephrosis
41. Prognosis cont Fetuses that present with these findings have a very poor prognosis
These die in the neonatal period from severe pulmonary hypoplasia
Normal fluid volume with stable hydronephrosis have better outcomes
Normal renal cortical echogenicity does not exclude renal dysplasia
42. Sonographic factors Good prog factors
Normal fluid
Diagnosis after 24 wk
Asymmetric hydronephrosis
Urinary ascites
Isolated Poor prog factors
Oligohydramnios
Diagnosis before 24 wks
Echogenic kidneys
Perinephric urinoma
Associated abnormalities
43. Urine Biochemistry
44. 6/19/03 � Bladder tap #1 Sodium - 116 mmol/L
Chloride - 92 mmol/L
U osm - 265
Protein - 112 mg/dl
Calcium - 8.5 mg/dl
45. 6/20/03 Bladder tap #2 Sodium - 114 mmol/L
Chloride - 90 mmol/L
U osm - 249
Protein - 95 mg/dl
Calcium - 9.2 mg/dl
46. 6/23/03 Bladder tap #3 Sodium - 118 mmol/L
Chloride - 93 mmol/L
U osm - 255
Protein - 113 mg/dl
Calcium - 8.1 mg/dl
47. Management Poor prognosis group � may offer termination because infants ultimately die of pulmonary hypoplasia � or offer conservative management
Fetuses with normal fluid and stable hydronephrosis � serial u/s until delivery
Poor or good prognosis � depends upon serial renal urine biochemistries
48. Management cont Fetuses with good prognosis � placement of vesicoamniotic shunt with Rodeck catheter (double pigtail)
Counsel re: rupture of membranes,infection, injury to fetus, intraplacental bleeding, PTL
High density plastic with open metal tipped proximal and distal ends placed at fundal region � best fetal position vertex, back down
Memory of the plastic allow return to shape
Follow with serial u/s to confirm placement
49. Management Cont Consultation with pediatric urologist
Route of delivery � routine obstetric indications
Average age of delivery due to spontaneous rupture of membranes = 33-35 wks
Following delivery � sterile ostomy bag to abdomen until renal function and anatomical evaluation by pediatric urologist
50. Summary PUVS � bladder outlet obstruction
Affects 1 in 5,000 � 8,000 boys
Etiology unknown
Obstruction of posterior urethra
Diagnosed by u/s
Prognosis � dependent upon severity of hydronephrosis and urine chemistries
51. References Ultrasound and Fetal Therapy, �fetal shunt procedures� Johnson M.P., Feldman and M.I. Evans; chapter 1
Bettelheim et al, Prenatal diagnosis of fetal urinary ascits, Ultrasound Obstetrics and Gynecology 2000; 16: 473-475
Sonographic Diagnosis of Fetal Medicine, 634 � 637.