Download
1 / 27
380 likes | 961 Views
Cytochrome P450 2C9. Curt Geier PharmD Candidate 2010 University of Washington School of Pharmacy . Outline. Introduction Case Examples of Interactions Significance of CYP2C9 Polymorphisms Narrow Therapeutic Index Drugs CYP2C9 and GeneMedRX. Introduction- What are CYP450s?.

E N D
Cytochrome P450 2C9 Curt Geier PharmD Candidate 2010 University of Washington School of Pharmacy
Outline • Introduction • Case Examples of Interactions • Significance of CYP2C9 • Polymorphisms • Narrow Therapeutic Index Drugs • CYP2C9 and GeneMedRX
Introduction-What are CYP450s? • Family of 40+ heme-protein enzymes in humans • Located in smooth endoplasmic reticulum of hepatocyte and luminal epithelium of small intestine • Catalyze “Phase I” metabolism • Generally transforming a compound into a more polar product to be excreted or passed on to Phase II metabolism. • Most commonly through a monooxygenase reaction2: • RH + NADPH + O2 + H+ROH + NADP+ + H20\ • 2. Block J, Beale J. Organic Medicinal and Pharmaceutical Chemistry 11th Ed. Lippincott Williams & Wilkins: 2004.
Introduction-2C9 • One of four functional 2C genes located on chromosome 10 (including 2C8, 2C18 and 2C19)9. • Responsible for metabolic clearance of ~15% of all drugs that undergo Phase I metabolism5. • It is one of the most abundant hepatic CYP enzymes with ~20% of CYP activity in the liver9. • 9. Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome P450 enzymes and its clinical impact. Drug Metabolism Reviews. 2009; 41(2):89-295 • 5. Rettie AE, Jones JP. Clinical and Toxicological Relevance of CYP2C9: Drug-Drug Interactions and Pharmacogenetics. Annu. Rev. Pharmacol. Toxicol. 2005;45:477-94
Introduction-2C9 Why is CYP 2C9 Clinically Significant? • 2C9 is responsible for metabolism of a large number of commonly utilized drugs. Greater than 100 substrates have been discovered9. • The enzyme is particularly susceptible to significant interactions because of its role in metabolizing low therapeutic index medications • Genetic polymorphisms are very prevalent • 9. Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome P450 enzymes and its clinical impact. Drug Metabolism Reviews. 2009; 41(2):89-295
Introduction-2C9 Common 2C9 Substrates (not all-inclusive) Losartan Phenobarbital Phenytoin Sulfa drugs Tamoxifen S-warfarin Torsemide • Indomethacin • Lornoxicam • Meloxicam • Suprofen • Temoxicam • Chlorpropamide • Glipizide • Glimepiride • Glyburide • Nateglinide • Rosiglitazole • Tolbutamide • Bosentan • Candesartan • Fluvastatin • Irbesartan • Fluoxetine • Sertraline • Valproic acid • Aceclofenac • Celecoxib • Diclofenac • Flurbiprofen • Ibuprofen
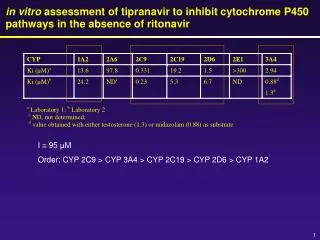
Introduction-2C9 CYP 2C9 Inhibitors7 Inhibition occurs rapidly once the inhibitor is present in the system • Fluconazole (Ki~7) • Fluvoxamine (Ki~6) • Gemfibrozil (Ki~5.8) • Sulfaphenazole, miconazole (Ki~0.3) • Amiodarone (desethylamiodarone), sertraline, sulfamethoxazole, valproic acid, voriconazole days • 7. Takanohashi T, Koizumi T, Mihara R, Okudaira K. Prediction of the Metabolic Interaction of Nateglinide with Other Drugs Based on in Vitro Studies. Drug Metab. Pharmacokinet. 2007;22(6):409-418
Introduction-2C9 CYP 2C9 Inducers Induction involves upregulation of the enzyme and takes longer than inhibition for effect • Rifampin • Aprepitant • Bosentan • Carbamazepine • Rifampin • Ritonavir • St. John’s Wort days
2C9 InteractionCase 1 • Teresa, a 29 year old female with a history of epilepsy stabilized on Dilantin 300mg/day for 3 years, is prescribed fluoxetine 20mg daily for depression. One week later she presents to the ER with persistent tremor and incessant headache, her total phenytoin concentration was shown to be 25.4mg/L. • The easiest drug interaction concept is also likely the most common. Fluoxetine is a moderate inhibitor of 2C9, but enough to make a significant change in metabolism of phenytoin. A small change in drug therapy can result in a large adverse drug event.
2C9 InteractionCase 2 • David, a 43 year old male with Type II DM and HTN is switched from lisinopril 10mg daily to losartan 50mg daily after complaining of a cough. The patient was increased to 100mg/day with little gain in BP control. Realizing the high cardiovascular risk in this patient, the clinician changed to candesartan at a moderate dose of 8mg daily. One week later the patient presents to clinic with severe light-headedness and orthostatic hypotension. • David was later discovered to be a CYP2C9*3*3 genotype and was not adequately activating the prodrug losartan. Additionally, candesartan is a 2C9 substrate. Candesartan exposure increases 100% in 2C9 IM patients, and likely even more in PM patients3. • 3. Kirchheiner J, Brockmoller J. Clinical Consequences of cytochrome P450 2C9 polymorphisms. Clinical Pharmacology and Therapeutics. 2005; 77(1): 1-16
2C9 InteractionCase 3 • Lewis, a 64 year old male with a history of HTN, previous DVT stabilized on warfarin 3mg/day, and depression managed with sertraline presents to the ER with shortness of breath and severe chest pain. The patient is diagnosed with a pulmonary embolism. Labs indicated his INR was 1.2. Upon questioning, his wife reports that he had been taking St. John’s Wort for the past month after he heard on the news that it can help with depression. • Lewis had been taking St. John’s Wort, a known enzyme inducer. CYP2C9, and 3A4, were induced leading to a subtherapeutic warfarin dose and INR. Clinicians should be sure to ask for any OTC medications or herbals that patients are taking.
Significance: Polymorphisms • Greater than 40% of individuals in white populations are carriers for a variant gene5. • Genotypic and phenotypic variants • 2C9*1- wild type enzyme • 2C9*2- small decrease in Vmax (0-35%), no change in Km5 • 2C9*3- significant decrease in Vmax, increase in Km results in clearance 15-20% of wild type enzyme8 • A total of 33 variants have been identified, most are rare9 • 5. Rettie AE, Jones JP. Clinical and Toxicological Relevance of CYP2C9: Drug-Drug Interactions and Pharmacogenetics. Annu. Rev. Pharmacol. Toxicol. 2005;45:477-94 • 8. Yasar U, Eliasson E, Dahl M, Johansson I, Ingelman-Sundberg M, Sjo¨qvist F. Validation of Methods for CYP2C9 Genotyping: Frequencies of Mutant Alleles in a Swedish Population. Biochemical and Biophysical Research Communications. 1999;254:628-631 • 9. Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome P450 enzymes and its clinical impact. Drug Metabolism Reviews. 2009; 41(2):89-295
Significance: Polymorphisms • Genotype Population Prevalence3 • 2C9*1*1 (wild type): • African- 87%, Asian- 96.5%, White- 65.3% • 2C9*1*2 (minor functional impairment) • African- 8.7%, Asian- 0%, White- 20.4% • 2C9*1*3 (moderate functional impairment) • African- 4.3%, Asian- 3.5%, White- 11.6% • 2C9*2*2 (0.9%) and 2C9*2*3 (1.4%) are generally only present in white populations and show moderate functional impairment. • 2C9*3*3 (severe functional impairment) • White- 0.4%, rare in other populations • 3. Kirchheiner J, Brockmoller J. Clinical Consequences of cytochrome P450 2C9 polymorphisms. Clinical Pharmacology and Therapeutics. 2005; 77(1): 1-16
Significance: Polymorphisms AUC of select drugs in 2C9 PM vs. NM patients Drug Exposure (AUC) 3 • 3. Kirchheiner J, Brockmoller J. Clinical Consequences of cytochrome P450 2C9 polymorphisms. Clinical Pharmacology and Therapeutics. 2005; 77(1): 1-16
Significance: Narrow Therapeutic Index Drugs • Therapeutic Index= (LD50/ED50) • Drugs that require close monitoring and small dosage adjustments can move from therapeutic to toxic • Particularly difficult for medications that are metabolized through pathways susceptible to genetic polymorphisms • Examples of narrow index medications (not 2C9) include digoxin, tricyclic antidepressants and aminoglycoside antibiotics
Significance: Narrow Therapeutic Index Drugs • S-warfarin (5-10x more active than r-warfarin) • Number 83 in top 200 most prescribed medications11 • Vitamin K epOxide Reductase (VKOR) inhibitor • Prevents synthesis of vitamin K dependent clotting factors • VKOR is also subject to genetic polymorphism (responsible for ~30% of variation) 6 • Phenocoumarol, acenocoumarol also metabolized by 2C9 • Primarily used for prevention of thromboembolic events in high risk patients • 11. Top 200 data from Rxlist.com • 6. Stehle S, Kirchheiner J, Lazar A, Fuhr U. Pharmacogenetics of oral anticoagulants: a basis for dose individualization. Clin. Pharmacokitetics 2008;47(9):565-94
Significance: Narrow Therapeutic Index Drugs • S-warfarin (cont.) • Monitored using PT/INR as opposed to serum levels. Because of polymorphisms intrapatient variability is large • INR therapeutic range for most indications is 2-3 with exception of patients with mechanical heart valves • INR>3 is associated with higher bleed risk, <2 associated with embolic risk • Compared to CYP2C9*1*1, CYP2C9*3*3 patients are estimated to require a lower warfarin dose by 3.3-fold6. • 6. Stehle S, Kirchheiner J, Lazar A, Fuhr U. Pharmacogenetics of oral anticoagulants: a basis for dose individualization. Clin. Pharmacokitetics 2008;47(9):565-94
Significance: Narrow Therapeutic Index Drugs • Phenytoin • Number 151 in top 200 most prescribed medications11 • Common antiepileptic medication useful in a variety of seizure disorders. Also a type IB antiarrhythmic. • Highly bound to albumin in serum, protein displacements may result in changes in efficacy as free phenytoin levels change • Metabolized primarily by 2C9 and 2C194 • Also an inducer of 2B6, 2C8, 2C9, 2C19 and 3A44 • 11. Top 200 data from Rxlist.com • 4. Phenytoin. UpToDate Online. Accessed via University of Washington on August 26th, 2009 at http://www.uptodate.com.offcampus.lib.washington.edu/online/content/topic.do?topicKey=drug_l_z/199700&selectedTitle=1~150&source=search_result#33.
Significance: Narrow Therapeutic Index Drugs • Phenytoin (cont.) • Monitored by serum levels. Therapeutic total serum concentrations generally 10-20mcg/ml1. • Unbound concentrations may be utilized in some cases. Therapeutic range 1-2mcg/ml1 • Concentrations >20mcg/ml are associated with tremor and headache. Greater than 40mcg/ml has resulted in drug-induced seizures and coma1. • CYP2C9*3*3 patients have >100% increase in exposure compared to *1*1 patients3. • 1. Bauer LA. Clinical Pharmacokinetics Handbook. McGraw Hill: Medical Publishing Division; 2006. • 3. Kirchheiner J, Brockmoller J. Clinical Consequences of cytochrome P450 2C9 polymorphisms. Clinical Pharmacology and Therapeutics. 2005; 77(1): 1-16
Significance: Narrow Therapeutic Index Drugs • Sulfonylureas(glimepiride, glipizide, glyburide, nateglinide*, tolbutamide) • All metabolized, to some degree, by CYP2C9 • Although not technically “narrow therapeutic index,” severe side effects can occur if concentrations vary too far • Stimulate beta cells to secrete insulin and reduces glucose output from the liver • Tolbutamide is not used often today due to a possible increased risk of cardiovascular mortality and side effects *-Nateglinide is a nonsulfonylureameglitinide derivative
Significance: Narrow Therapeutic Index Drugs • Sulfonylureas(cont.) • Symptoms of increased concentrations are mostly mechanism driven, with hypoglycemia causing the most danger. • CYP2C9*3*3 genotype patients show an increased exposure by 460% for glipizide, and 100% for glyburide an nateglinide as compared to CYP2C9*1*1 patients3. • Glimepiride exposure increases >100% in 2C9*1*3 (IM) patients, no data is available for PM patients3. • 3. Kirchheiner J, Brockmoller J. Clinical Consequences of cytochrome P450 2C9 polymorphisms. Clinical Pharmacology and Therapeutics. 2005; 77(1): 1-16
2C9 and GeneMedRX Drugs for which 2C9 polymorphism data is entered Irbesartan Lornoxicam Losartan Nateglinide Phenytoin Piroxicam S-warfarin Tenoxicam Tolbutamide Torsemide • Acenocoumarol • Candesartan • Celecoxib • Diclofenac • Flurbiprofen • Fluvastatin • Glimepiride • Glipizide • Glyburide • Ibuprofen
2C9 and GeneMedRXQuality Assessment and Updates Portion of data predicted by GeneMedRX that is consistent with literature for 2C9 PM patients (n=16) • Percentage of polymorphism-drug interaction predictions that: • Overestimated Reduction- 19% • Underestimated Reduction- 56% • Correctly Predicted Reduction- 25% • The program severely (by more than 1 “class”) overestimated in one case, and severely underestimated in two cases. • Example- If the actual reduction was >150%, and the predicted reduction was 25-75% • Data from GeneMedRX.com
2C9 and GeneMedRXQuality Assessment and Updates Portion of data predicted by GeneMedRX that is consistent with literature for 2C9 IM patients (n=16) • Percentage of polymorphism-drug interaction predictions that: • Overestimated Reduction- 6% • Underestimated Reduction- 38% • Correctly Predicted Reduction- 56% • There were no incorrect predictions outside of 1 class • Data from GeneMedRX.com
Conclusion • Clinicians often opt to switch to more costly, and less efficacious therapy when a patient experiences an adverse drug event when commonly the cause, unknown to the clinician, is a drug interaction. • Additionally, many serious side effects could be prevented through knowledge of metabolism pathways, drug interactions and genetic polymorphisms. • Because of the novelty of gene-drug interaction information, resources should be made available (i.e. GeneMedRX, trained PharmD students) and should be utilized by clinicians, particularly those unfamiliar with drug and genotypic interactions. • CYP2C9 is one of many clinically important enzyme with many significant interactions that should be considered when choosing therapy. • Drug and genetic interactions are not contraindications to therapy. They are predictable and manageable if recognized in a timely matter.
References • 1. Bauer LA. Clinical Pharmacokinetics Handbook. McGraw Hill: Medical Publishing Division; 2006. • 2. Block J, Beale J. Organic Medicinal and Pharmaceutical Chemistry 11th Ed. Lippincott Williams & Wilkins: 2004. • 3. Kirchheiner J, Brockmoller J. Clinical Consequences of cytochrome P450 2C9 polymorphisms. Clinical Pharmacology and Therapeutics. 2005; 77(1): 1-16 • 4. Phenytoin. UpToDate Online. Accessed via University of Washington on August 26th, 2009 at http://www.uptodate.com.offcampus.lib.washington.edu/online/content/topic.do?topicKey=drug_l_z/199700&selectedTitle=1~150&source=search_result#33. • 5. Rettie AE, Jones JP. Clinical and Toxicological Relevance of CYP2C9: Drug-Drug Interactions and Pharmacogenetics. Annu. Rev. Pharmacol. Toxicol. 2005;45:477-94 • 6. Stehle S, Kirchheiner J, Lazar A, Fuhr U. Pharmacogenetics of oral anticoagulants: a basis for dose individualization. Clin. Pharmacokitetics 2008;47(9):565-94 • 7. Takanohashi T, Koizumi T, Mihara R, Okudaira K. Prediction of the Metabolic Interaction of Nateglinide with Other Drugs Based on in Vitro Studies. Drug Metab. Pharmacokinet. 2007;22(6):409-418 • 8. Yasar U, Eliasson E, Dahl M, Johansson I, Ingelman-Sundberg M, Sjo¨qvist F. Validation of Methods for CYP2C9 Genotyping: Frequencies of Mutant Alleles in a Swedish Population. Biochemical and Biophysical Research Communications. 1999;254:628-631 • 9. Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome P450 enzymes and its clinical impact. Drug Metabolism Reviews. 2009; 41(2):89-295 • 10. Drug Structures from Drugs.com Accessed August 25, 2009 from http://www.drugs.com • 11. Top 200 data from Rxlist.com
Questions? Thank you