Download
1 / 140

E N D
Oncostomatology: statistics, organization of medical service, centre system of health. Classification of tumors of maxillofacial area. High qualities tumors and tumor-like formations of soft tissue of maxillofacial area (papilloma, fibroma, lіpoma, hemangіoma, ateroma, neyrofіbromatozis, cysts of soft tissue): etiology, pathogenesis, histological structure, clinic, differential diagnostics, treatment and prophylaxis of complications.
Traumatic (Irritation) Fibroma: Clinical Features • Traumatic fibromas appear as firm, asymptomatic nodules covered by epithelium unless secondarily traumatized. • They usually occur along the line of occlusion in the lower lip or buccal mucosa; they may, however, be found anywhere in the oral cavity. • These lesions, which are reactive hyperplasias rather than true neoplasms as suggested by the term fibroma, are very common oral lesions.
Traumatic (Irritation) Fibroma: Cause • It is a reactive lesion to trauma or chronic irritation. • Although rare according to research studies, clinically similar lesions may be true neoplasms (fibromas).
Traumatic (Irritation) Fibroma: Treatment • Surgical excision is the treatment of choice.
Traumatic (Irritation) Fibroma: Significance • This lesion is a reactive one which has limited growth potential. • No malignant transformation has been reported.
Epulis Fissuratum Denture Injury Tumor Inflammatory Fibrous Hyperplasia Denture Epulis
Epulis Fissuratum: Clinical Features • Tumor-like hyperplasia of fibrous connective tissue associated with denture flange. • Presents as fold (s), usually two, with flange fitting in between. • The lesion is usually firm and fibrous but may show erythema and ulceration. • Most common on facial aspect in the anterior of either jaw. • It is more common in middle-aged and older females (two-thirds to three-fourths of the cases are in females).
Epulis Fissuratum: Cause • Chronic irritation or trauma from denture flange making the lesion a reactive hyperplasia. • The denture is typically ill-fitting.
Epulis Fissuratum: Treatment • Treatment consists of surgical removal of excess tissue with microscopic examination and…. • The poorly fitting denture should be remade or relined.
Epulis Fissuratum: Significance • Lesion will recur (or remain) if ill-fitting denture is not remade or relined.
Papillary Hyperplasia Inflammatory Papillary Hyperplasia Palatal Papillomatosis Denture Papillomatosis
(Inflammatory) Papillary Hyperplasia: Clinical Features • Papillary hyperplasia is a reactive tissue growth that usually, but not always, develops beneath a denture. • It typically appears as a painless, papillomatous, “cobblestone” lesion of hard palate although occasionally it occurs on the edentulous mandibular ridge or in association with epulis fissuratum. • The lesion is usually asymptomatic and red because of inflammation. • It is a common lesion in denture wearers.
Papillary Hyperplasia: Cause • Soft tissue reaction to ill-fitting denture and probable fungal overgrowth. • Patients generally have poor oral/denture hygiene. • One study indicated approximately 20 % of the patients wore their dentures 24 hours per day.
Papillary Hyperplasia: Treatment • In cases of very early inflammatory papillary hyperplasia, removal of the denture may allow the erythema and edema to subside and the tissues may resume a more normal appearance. • Lesions may show some improvement after topical or systemic antifungal therapy. • For advanced cases, excision of the lesion is treatment of choice prior to the fabrication of a new denture. • Partial and full-thickness surgical blade excision, curettage, electrosurgery and cryrosurgery have all been used with success in particular cases.
Papillary Hyperplasia: Significance • The lesion is not premalignant. • Following surgery the old denture can be lined with a temporary tissue conditioner that acts as a dressing and promotes healing. • After healing, the patient should be encouraged to leave the new denture out at night and to practice good denture hygiene.
Peripheral Giant Cell Granuloma Giant Cell Epulis
Peripheral Giant Cell Granuloma: Cause • This is a reactive lesion associated with chronic trauma or irritation.
Peripheral Giant Cell Granuloma: Treatment • Excision is the treatment of choice down to the underlying bone. • Adjacent teeth should be carefully scaled to remove any source of irritation thus minimizing the risk of recurrence.
Peripheral Giant Cell Granuloma:Significance • These lesions will remain indefinitely if not treated. • Remember, it is a reactive lesion similar in clinical appearance to the pyogenic granuloma.
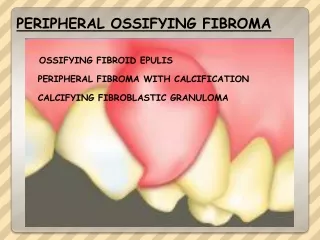
Peripheral Ossifying Fibroma Ossifying Fibroid Epulis Peripheral Fibroma with Calcification Calcifying Fibroblastic Granuloma
Peripheral Ossifying Fibroma (POF) • The POF is a common reactive gingival growth. • Its pathogenesis is best describe as uncertain; some POFs have been suggested to develop from pyogenic granulomas. • It should be noted that POFs are not the same as peripheral odontogenic fibromas and they are not the soft tissue counterpart of the central ossifying fibroma.
Peripheral Ossifying Fibroma (POF): Clinical Features • This lesion occurs exclusively on the gingiva. • It appears as a nodular mass usually arising from the interdental papilla area. • It is red to pink in color and the surface is often ulcerated. • POFs are more common in young adults and females. • There is a slight predilection for the maxilla and the anterior region of the jaws.
Peripheral Ossifying Fibroma: Treatment and Prognosis • The treatment of choice is local surgical excision down to the periosteum to prevent recurrence. • The adjacent teeth should be scaled to eliminate irritants such as calculus. • A recurrence rate of 16 % has been reported in the literature.
Hemangioma and Vascular Malformations • The term hemangioma has traditionally been used to describe a variety of developmental vascular anomalies. • Currently, hemangiomas are considered to be benign tumors of infancy that are characterized by a rapid growth phase with endothelial cell proliferation, followed by a gradual involution. Most cannot be recognized at birth but make their appearance in most instances during the first 8 weeks of life. • Vascular malformations are structural anomalies of blood vessels without endothelial proliferation and are present at birth and persist throughout life.
Hemangioma • Hemangiomas are the most common tumors of infancy. • They have a female gender predilection (3:1) and are most common in the White population. • 60% of the hemangiomas occur in the head and neck region with 80% of them occurring as single lesions. Multiple lesions may be part of a syndrome. • About 50 % of all hemangiomas will show complete resolution by 5 years of age.
Vascular Malformations • These lesions are present from birth and persist throughout life. • As with hemangiomas, these lesions tend to darken with age. • Low-flow venous malformations typically have a blue color and are easily compressible. • Arteriovenous malformations are high-flow lesions that result from persistent direct arterial and venous communications. A palpable thrill or bruit is often noticeable and the overlying skin typically feels warmer to the touch.
Hemangioma and Vascular Malformations • Because most hemangiomas undergo involution, management often consists of “watchful neglect”. For problematic hemangiomas, surgical resection or pharmacologic therapy may be indicated (systemic steroids or interferon-α-2a). Flashlamp-pulsed dye lasers can be effective in treating port wine stains. • Management of vascular malformations depends on their size, location and associated complications. Sclerotherapy and surgical excision are the mainstays. • Treatment of arteriovenous malformations is more challenging and may involve surgical resection or embolization. • Central vascular malformations of the jaws are potentially dangerous lesions because of severe bleeding. Needle aspiration of any undiagnosed intrabony lesion before biopsy is a wise precaution to rule out these lesions.