Download

1 / 66
700 likes | 1.08k Views
Endocrine resistance: molecular pathways and rational development of targeted therapies Grazia Arpino Università di Napoli Federico II. Enhancing Endocrine Therapy for Breast Cancer. Current Endocrine Therapy : Tamoxifen ; aromatase inhibitors

E N D
Endocrine resistance: molecular pathways and rational development of targeted therapies Grazia Arpino Università di Napoli Federico II
Enhancing Endocrine Therapy for Breast Cancer • Current Endocrine Therapy: • Tamoxifen; aromataseinhibitors • Limitedby “de-novo” or “acquired” endocrine resistance • De Novo/AcquiredEndocrine Resistance: • ER expression & function • RoleofGrowthFactorReceptors (EGFR/HER2) in “Cross-Talk” • Downstream intracellularsignaling (ie. mTor, MAPK vs AkT) • SignalTransductionInhibitors, biology and clinicalrole: • EGFR – erlotinib, gefitinib • HER2 – trastuzumab, lapatinib • mTOR – everolimus, temsirolimus
Enhancing Endocrine Therapy for Breast Cancer • Current Endocrine Therapy: • Tamoxifen; aromataseinhibitors • Limitedby “de-novo” or “acquired” endocrine resistance • De Novo/AcquiredEndocrine Resistance: • ER expression & function • RoleofGrowthFactorReceptors (EGFR/HER2) in “Cross-Talk” • Downstream intracellularsignaling (ie. mTor, MAPK vs AkT) • SignalTransductionInhibitors, biology and clinicalrole: • EGFR – erlotinib, gefitinib • HER2 – trastuzumab, lapatinib • mTOR – everolimus, temsirolimus
Enhancing Endocrine Therapy for Breast Cancer • Current Endocrine Therapy: • Tamoxifen; aromataseinhibitors • Limitedby “de-novo” or “acquired” endocrine resistance • De Novo/AcquiredEndocrine Resistance: • ER expression & function • RoleofGrowthFactorReceptors (EGFR/HER2) in “Cross-Talk” • Downstream intracellularsignaling (ie. mTor, MAPK vs AkT) • SignalTransductionInhibitors, biology and clinicalrole: • EGFR – erlotinib, gefitinib • HER2 – trastuzumab, lapatinib • mTOR – everolimus, temsirolimus
~5 years tamoxifenvs Not, ER+ patients 10% 5 years of adjuvant tamoxifen safely reduces 15-year risks of breast cancer recurrence and death EBCTGC, Lancet 2011
E2 E2 E2 MechanismofAction-Tamoxifen Protein CoA Transcription mRNA + ER ER CoR CoA ERE Promoter Gene ER ER ERE Gene + Tam Tam Tam CoR Transcription ER ER ERE Promoter Gene
~5 years tamoxifenvs Not, ER+ patients 25% However, almost one quarter of the patients with ER+ tumor develop resistance EBCTGC, Lancet 2011
Major Problem (Endocrine Therapy) Resistance De Novo Acquired
Her2+ Better Her2+ worse Overall 1.44 (1.34 – 1.56) MetanalysisER+Patients (N=1195) Relative Risk of Treatment Failure (95%CI) Ellegde 1.21 (0.87 – 1.69) Hayes 1.06 (0.47 – 2.38) Houston 2.07 (1.57 – 2.73) Lipton 1st 1.42 (1.24 – 1.63) Lipton 2nd 1.40 (1.25 – 1.56) Willsher 1.33 (0.56 – 3.16) Wright 1.54 (0.86 – 3.74) Yamauchi 1.66 (1.05 – 2.64) De Laurentiis M., et al.Clin.Cancer Res., 2005.
In Vivo Model of Tamoxifen Resistance Tumorvolume(mm3) De Novo Tam-R 1200 Tam-S Acquired Tam-R 1000 800 600 Tam 400 MCF7 200 MCF7 / HER2 0 0 21 49 77 105 Days Osborne et al. JNCI 1994
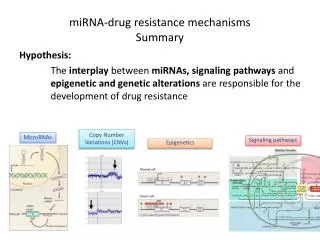
Genomic & non-genomic ER cross-talk P P P EGFR HER2 IGFR Cell stress cytokines E2 Basal transcription machinery CBP p160 ER ER E2
Genomic & non-genomic ER cross-talk P P P EGFR HER2 IGFR Cell stress cytokines Ras Rac-1 SOS Grb2 CDC42 ER Raf PI3k MEKK1 MEK1/2 MLK3 ERK1/2 AKT p60rsk p38 MKK3/6 mTor ER Bad ER ER Basal transcription machinery CBP p160 ER ER E2
Genomic & non-genomic ER cross-talk P P P EGFR HER2 IGFR Cell stress cytokines Ras Rac-1 SOS Grb2 CDC42 ER Raf PI3k MEKK1 MEK1/2 MLK3 ERK1/2 AKT p60rsk p38 MKK3/6 mTor ER Bad ER E2 ER Basal transcription machinery CBP p160 ER ER E2
800 E2 MCF7/HER2 Tumors Tam 600 Tumor Volumes (mm3) 400 Tam+Gef Tam+P Tam+T 200 0 1 21 42 63 84 105 126 147 168 189 209 Days Hypothesis:Resistanceis due to incomplete blockade of the HER signaling pathway (all HER dimer pairs). Effect of HER Family Inhibitors on Tam-Stimulated Growth Arpino, JNCI 2007
TanDEM Study Design Anastrozole 1 mg daily +Trastuzumab 4 mg/kg Loadingdose 2 mg/kg qwuntildiseaseprogression HER2-positiveHR-positive MBC(n=208) R Anastrozole1 mg untildiseaseprogression Crossover to receive trastuzumab was actively offered to all patients who progressed on anastrozole alone HR, hormonereceptor MBC, metastaticbreastcancer R, randomisation Kaufman et al, JCO 2009
TanDEM Progression-free Survival 1.0 0.8 Events 8799 Median PFS 4.8 months2.4 months 95% CI 3.7, 7.02.0, 4.6 p value 0.0016 0.6 Probability 0.4 0.2 0 5 10 16 20 25 30 35 40 45 50 55 60 Months No. at risk A + H A 103 104 48 36 31 22 17 9 14 5 13 4 11 2 9 1 4 0 1 0 1 0 0 0 0 0 Kaufman et al, JCO 2009
EGF30008 – Study Design Patient Population R A N D O M I Z E Letrozole 2.5 mg daily+Placebo • ER+/PgR+ (HR+) • Postmenopausal • HER2+, HER2- or unknown • Stage IIIb/IIIc, IV • No prior treatment for MBC Stratification • Diseasesites • Boneonly/othesites • Intervalsinceprioradjuvantanti-estrogentherapy • < 6 mo / ≥ 6 mo or None Letrozole 2.5 mg daily+Lapatinib 1500 mg daily n = 1286 pts (including n=219 HER2+) Johnston S, et al JCO2009
ELECTRA – Study Design R A N D O M I Z E Letrozole 2.5 mg daily+Placebo PatientPopulation • ER+/PgR+ (HR+) • Postmenopausal • HER2+, • No prior treatment for MBC Letrozole 2.5 mg daily+Trastuzumab HuoberBreast 2009
ELECTRA – Study Design *hazard ratio 0.67; p = 0.23 ** odds ratio 2.99, 95% CI 1.01-8.84 HuoberBreast 2012
Trastuzumab Pertuzumab HER4 ? Lapatinib Gefitinib HER Family Inhibitors EGF TGFα Heregulin HER2 HER2 EGFR HER3 X Tumor growth and survival
Effect of HER Family Inhibitors on Tam-Stimulated Growth 800 Complete Responses Tam+P 5/18 Tam+P+T 12/18 Tam+P+T+G 18/20 E2 Tam 600 Tumor Volumes (mm3) 400 Tam+P Tam+P+T 200 Tam+P+T+G 0 1 21 42 63 84 105 126 147 168 189 209 Days Arpino, JNCI 2007
MCF7/HER2-18 Effect of HER Family Inhibitors on Estrogen Deprivation 1000 Complete Regression ED+T 4/13 ED+L 5/13 ED+L+T 11/13 800 ED 600 Tumor Volume (mm3) 400 ED+L 200 ED+T ED+L+T 0 50 100 150 200 250 Treatment Days Rimawi Cancer res in press
Lapatinib (1000 mg/day) Surgery Trastuzumab (4 mg/kg load, 2 mg/kg q-weekly) Weeks TBCRC 006: Neoadjuvant Lapatinib & TrastuzumabWithout Chemotherapy Bx 8 12 0 2 Lap (L) + Tras (T) + Endocrine Rx if ER+
Pathologic Response pCR rates: 18/61 (30%) • ER pos: 8/39 (21%) • ER neg: 10/22 (46%) pCR+npCR rates: 34/61 (56%) • ER pos: 22/39 (56%) • ER neg: 12/22 (55%)
PERTAIN Investigational arm [Arm A] Pertuzumab + trastuzumab Until disease progression, unacceptable toxicity, withdrawal of consent, or death + Patients with HER2- and hormone receptor-positive advanced breast cancer not previously treated with systemic non-hormonal anticancer therapy in the metastatic setting (n ~250) AI or Patients receiving induction chemotherapy (investigator’s discretion) AI Docetaxel or paclitaxel (starting after induction chemotherapy phase) Up to 18 weeks Up to 18 weeks R Control arm [Arm B] Trastuzumab Until disease progression, unacceptable toxicity, withdrawal of consent, or death + AI or Patients receiving induction chemotherapy (investigator’s discretion) AI Docetaxel or paclitaxel (starting after induction chemotherapy phase)
In Vivo Model of Tamoxifen Resistance Tumorvolume(mm3) De Novo Tam-R 1200 Tam-S Acquired Tam-R 1000 800 600 Tam 400 MCF7 200 MCF7 / HER2 0 0 21 49 77 105 Days Osborne et al. JNCI 1994
Acquired Endocrine Resistance • ER signalingsurvivers: • ER expressed, althoughfunctionmaychange • Enhance ER activation • Reversiblesilencingof ER can alsooccur • Enhancedgrowthfactorsignaling (EGFR, HER2) occurs: • Cross-talkbetween GFR and ER: • activationofgenomic ER via AkT/MAPK inducedphosphorylation • non-genomicassociationof ER with HER2 / EGFR / IGFR • mTORpathwayactivationdisregulating ER genomicfunction
Fulvestrant: selectiveestrogenreceptordownmodulator • Pure estrogenreceptorantagonist: • - high affinityforestrogenreceptor • - downregulates ER and blocks ER- mediatedtranscription • - downregulatesPgR • Pre-clinical and clinicalstudiesshowed: • - Fulvestrantiseffective in tamoxifen-resistanttumors • Indications: • - MBC progressingafterotherantiestrogentherapy in • postmenopausal women
SWOG 0226: Progression-Free Survival All eligible patients (n=694) 1.00 Anastrozole + Fulvestrant (268 events) Anastrozole (297 events) Stratified log-rank p = 0.0070 0.75 Median PFS Anastrozole 13.5 mos (95% CI 12.1-15.1) Combination 15.0 mos (95% CI 13.2-18.4) 0.50 0.25 HR = 0.80 (95% CI 0.68-0.94) 0.00 0 12 24 36 48 60 72 Months since registration N at risk AN AN + FV 349 345 199 193 114 92 53 39 21 11 8 3 2 0
SWOG 0226: Progression-Free Survival Prior adjuvant tamoxifen (n=280) 1.00 Anastrozole + Fulvestrant (114 events) Anastrozole (119 events) Log-rank p = 0.037 0.75 Median PFS Anastrozole 14.1 mos (95% CI 12.0-16.8) Combination 13.5 mos (95% CI 11.0-19.3) 0.50 0.25 HR = 0.89 (95% CI 0.69-1.15) 0.00 0 12 24 36 48 60 72 Months since registration N at risk AN AN + FV 141 139 74 80 43 32 17 17 5 3 2 1 1 0
SWOG 0226: Progression-Free Survival No prior adjuvant tamoxifen (n=414) 1.00 Anastrozole + Fulvestrant (154 events) Anastrozole (178 events) Log-rank p = 0.0055 0.75 Median PFS Anastrozole 12.6 mos (95% CI 11.2-15.6) Combination 17.0 mos (95% CI 13.8-19.9) 0.50 0.25 HR = 0.74 (95% CI 0.59-0.92) 0.00 0 12 24 36 48 60 72 Months since registration N at risk AN AN + FV 208 206 125 113 71 60 36 22 16 8 6 2 1 0
SWOG 0226: Overall Survival All eligible patients (n=694) 1.00 Median OS Anastrozole 41.3 mos (95% CI 37.2-45.0) Combination 47.7 mos (95% CI 43.0-55.7) 0.75 0.50 HR = 0.81 (95% CI 0.65-1.00) 0.25 Anastrozole + Fulvestrant (154 deaths) Anastrozole (176 deaths) Stratified log-rank p = 0.049 0.00 0 12 24 36 48 60 72 Months since registration N at risk AN AN + FV 349 345 315 306 259 239 145 136 62 54 26 22 4 4
SWOG 0226: Overall Survival Prior adjuvant tamoxifen (n=280) 1.00 Median OS Anastrozole 44.5 mos (95% CI 38.0-54.8) Combination 49.6 mos (95% CI 37.9-71.2) 0.75 0.50 HR = 0.91 (95% CI 0.65-1.28) 0.25 Anastrozole + Fulvestrant (63 deaths) Anastrozole (68 deaths) Log-rank p = 0.59 0.00 0 12 24 36 48 60 72 Months since registration N at risk AN AN + FV 141 139 125 125 101 100 54 59 28 24 13 10 3 2
SWOG 0226: Overall Survival No prior adjuvant tamoxifen (n=414) 1.00 Median OS Anastrozole 39.7 mos (95% CI 33.1-43.9) Combination 47.7 mos (95% CI 43.4-58.3) 0.75 0.50 HR = 0.74 (95% CI 0.56-0.98) 0.25 Anastrozole + Fulvestrant (91 deaths) Anastrozole (108 deaths) Log-rank p = 0.0362 0.00 0 12 24 36 48 60 72 Months since registration N at risk AN AN + FV 208 206 190 181 158 139 91 77 34 30 13 12 1 2
Acquired Endocrine Resistance • ER signalingsurvivers: • ER expressed, althoughfunctionmaychange • Enhance ER activation • Reversiblesilencingof ER can alsooccur • Enhancedgrowthfactorsignaling (EGFR, HER2) occurs: • Cross-talkbetween GFR and ER: • activationofgenomic ER via AkT/MAPK inducedphosphorylation • non-genomicassociationof ER with HER2 / EGFR / IGFR • mTORpathwayactivationdisregulating ER genomicfunction
Changes of ER and PgRExpression in Primary vs. Subsequent Metestatic Disease Curiglianoet al. Ann. Onc. 2011
The discordance rates for ER, PgR, and HER2 status between primary tumor and liver metastases were 14.5%, 48.6%, and 13.9%, respectively, which led to change in therapy for 31 of 255 patients (12.1%). Rebiopsy??……YESifitsafe! Curiglianoet al. Ann. Onc. 2011
Changes in Molecular Profile Subtype at the Development of Endocrine Resistance Creighton et al Cancer Res. 2009
ER+veTamoxifen Resistance Cells (TAM-R) show Increased EGFR Signaling WT TAM-R p-EGFR p-HER2 p-ERK 1/2 Total-ERK 1/2 p-ERK 1/2 Knowldenet al. Endocrinology 2003
Changes in Growth Factor Receptor Expression and ER Activation in Acquired TamRvs WT cell lines Type I growth factor receptors(EGFR, ERBB2, ERBB3, ERBB4) WT TamR WT TamR p EGFR p ERK 1/2 Ras SoS EGFR ERK 1/2 p ERBB2 Raf PI3K ERBB2 pAKT (ser173) MEK AKT ERBB3 MAPK Akt ERBB4 pERa (ser118) p90RSK pERa (ser167) Basal transcription machinery Actin P P P p160 CBP ER ER total ERa ERE Target gene Pancholiet al. EndocrRelatCancer 2008
Tamoxifen +Gefitinib(n = 105) Tamoxifen +Placebo(n = 101) Median PFS (months) 10.9 8.8 HR of gefitinib to placebo = 0.84 (0.59, 1.18) HER2+ subset (n=37)Median PFS (months) 6.7 5.8 HR of gefitinib to placebo = 0.54 (0.25, 1.15) 1839IL/0225 – A randomised phase II study of Tamoxifen± Gefitinib in patients with ER+ve metastatic breast cancer Time to Progression STRATUM 1: (Endocrine Naive or > 12 m post adjuvant tamoxifen) 1.0 0.8 0.6 Proportion progression-free 0.4 0.2 0.0 0 100 200 300 400 500 600 700 800 900 1000 1100 Treatment Group time (days) tamoxifen + gefitinib tamoxifen + placebo Osborne et al. CCR 2010
Randomised phase II study of Anastrozole± Gefitinib in patients with ER+ve metastatic breast cancer Anastrozole +Gefitinib(n = 43) Anastrozole +Placebo(n = 50) 1.0 Events Median PFS (months) 22 14.5 32 8.2 0.8 HR (95% CI) = 0.55 (0.32, 0.94) 0.6 Probability of PFS 0.4 0.2 0.0 0 3 6 9 12 15 18 21 24 25 28 Months At risk Placebo Gefitinib 50 43 35 40 23 28 13 22 9 13 6 10 5 6 3 3 1 2 1 Cristofanilliet al. CCR2012
EGF30008 Progression-Free Survival: ITT and HER2-ve Populations HER2-ve * ITT *Centrally confirmed
EGF30008 PFS: HER2-ve Patients (N=952) • ≥ 6 Mo Since D/C of Tam (33%) or No Tam (67%) • Median tam duration 5 y • Median time since d/c 3.5 y • < 6 Mo Since D/C of Tam • Median tam duration 2.8 y • Median time since d/c 1 mo
2x2 Factorial Design Over Trial Design