Download
1 / 19
290 likes | 743 Views
Management of Critical Limb Ischemia. From ACC/AHA Guidelines for the Management of PAD. Critical Limb Ischemia. 5 P Pain Pulselessness Pallor Paresthesia Paralysis. Medical treatment. Class III PentoxifyllineI(Trental) is not useful. Class IIb

E N D
Management of Critical Limb Ischemia From ACC/AHA Guidelines for the Management of PAD
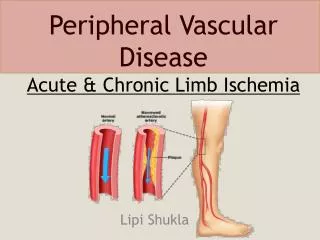
Critical Limb Ischemia 5P • Pain • Pulselessness • Pallor • Paresthesia • Paralysis
Medical treatment Class III PentoxifyllineI(Trental) is not useful. Class IIb IV PGE-1, or iloprost for 7~28 days reduce ischemic pain and facilitate ulcer healing, limited to small percentage of patients
Endovascular Treatment Class I 1.Treat inflow lesions first 2.Treat outflow lesions if infection or symptoms persisted 3.Use vasodilator for augmentation of intra-arterial pressure measurement
Thrombolysis Class I Catheter-based thrombolysis , with acute limb ischemia of less than 14 days Class IIa Mechanical thrombectomy, for adjunctive therapy Class IIb more than 14 days
Surgery for Critical Limb Ischemia Patients with CLI in whom open surgical repair is anticipated should undergo assessment of cardiovascular risk.
Consideration of surgery • Relief of rest pain • Healing of ulcers • Prior revascularization attempts • The type of procedure • The patient’s overall ability to recover
Primary amputation • Significant necrsis of weight-bearing portions of the foot • Uncorrectable flexion contracture • Paresis of the extremity • Refractory ischemic rest pain • Sepsis • Limited life expectancy
Aortoiliac Occlusive Disease • Aortobifemoral bypass • Iliac endarterectomy, patch angioplasty, or aortoiliac or iliofemoral bypass • Axillofemoral-femoral bypass • Vein > Prosthetic conduit • Patency of prosthesis below knee ↓
Infrainguinal Disease • Bypass to the above-knee or below-knee popliteal a. with autogenous v. • The point of origin for bypass: stenosis < 20%, most distal a. • Femoral-tibial a. bypass with v.
Infrainquinal disease • Composite sequential femoropopliteal-tibial bypass, and bypass to an isolated popliteal a. segment • Prosthetic femoral-tibial bypass Class IIa Prosthetic below-knee popliteal artery bypass
Post surgical care • Maximal cardiovascular ischemic risk reduction therapies • Bypass all major distal stenoses and occlusions if symptoms persisted. • F/U at least 2 years, Duplex for vein grafts ABI for synthetic grafts (0.9~1.3)
Cardiovascular Risk Reduction a. Lipid-Lowering Drugs b. Antihypertensive Drugs c. Diabetes Therapies d. Smoking Cessation e. Homocysteine-Lowering Drugs f. Antiplatelet and Antithrombotic Drugs
Lipid-Lowering Drugs Class I: Statin, LDL < 100 Class Iia Statin, LDL < 70 (high risk patients) Fibric acid derivative
Antihypertensive Drugs Class I BP < 140/90 < 130/80 (DM, CRD) Beta blockers are not contraindicated. Class IIa ACEI: reduce risk of cardiovascular disease for symptomatic patients
Diabetes Therapies Class I Foot care Class IIa HbA1c < 7%, for improve cardiovascular outcome reduce microvascular complication
Smoking Cessation Class I Comprehensive smoking cessation intervention
Homocysteine-Lowering Drugs Class IIb Folic acid and Vit.B12: for homocysteine > 14 μmole/l patients
Antiplatelet and Antithrombotic Drugs Class I Aspirin 75~325mg qd Clopidogrel 75mg qd reduce risk of MI, stroke, or vascular death Class III Warfarin is not indicated.