Download
1 / 49
590 likes | 946 Views
Clinical Documentation Improvement – Telling The Patient Story Thru ICD-10. Presented by: Karen Kvarfordt, RHIA, CCS-P, CCDS President, DiagnosisPlus, Inc. ICD-10 Changes Everything!.

E N D
Clinical Documentation Improvement – Telling The Patient Story Thru ICD-10 Presented by: Karen Kvarfordt, RHIA, CCS-P, CCDS President, DiagnosisPlus, Inc.
ICD-10 Changes Everything! It will change the way in which we document patient care in our medical records both in the hospital and in our practices. Patient’s story will be better told through better documentation!
ICD-10 • WHO (World Health Organization) owns & publishes ‘ICD’ (International Classification of Diseases). • WHO endorsed ICD-10 in 1990; members began using ICD-10 or modifications in 1994. • United Statesis the only industrialized country notusing ICD-10 for our coding & reporting of diseases, illnesses, and injuries. Why? What makes us so different?
Countries Using ICD-10 For Case Mix • United Kingdom (1995) • Denmark, Finland, Iceland, Norway, Sweden (1994 – 1997) • France (1997) • Australia (1998) • Belgium (1999) • Germany (2000) • Canada (2001) • United States (2015) • (Reimbursement+ Case Mix)
What is ICD-10? • Currently the U.S. health care industry uses ICD-9-CM codes for identifying and reporting diagnoses and procedures. • ICD-10 will replace the existing ICD-9 code sets (diagnosis & procedure) effective October 1, 2015. • ICD-10-CM = Diagnosis codes • ICD-10-PCS = Inpatient hospital procedure codes only • No impact on CPT and/or HCPCS codes! • CPT and HCPCS codes will continue to be used for physician and outpatient services including physician hospital visits (Observation & Inpatient) = E&M
Why Should We Do ICD-10? • What is the benefit to the provider? • Dramatic improvement in the assignment of costs to procedures performed. • ICD-10 will allow us to develop meaningful estimates about what a disease state or a procedure costs us, while ICD-9 is limited in what it can do in this regard. • Identify opportunities to avoid cost & improve lives. • Additional information in an ICD-10 diagnosis code includes severity and specific comorbidity, but it can also include information about demographics and some of the underlying reasons for the diagnosis.
Additional Benefits… • Share higher-quality data with other health care providers. • ICD-10 increases the amount of “specific” information in every diagnosis code and makes this more valuable to other providers. • For example, ICD-9 has a code for laceration of an artery. • ICD-10 lets you know if that artery was in someone’s finger or in their heart.
Reimbursements will better align with activity & cost. • Payers will reimburse severe & complex cases better and simple cases at lower rates. • How? By the diagnosis codes!
Here’s an Example • Imagine you had a patient who was noncompliant with their medical therapy. • In ICD-9, the only code we have available is V15.81 (personal history of noncompliance with medical treatment). • Is the patient noncompliant because of their own personal reason? Or something else?
How Will it Look in ICD-10? • Z9111 (Patient’s noncompliance with dietary regimen) • Z91120 (Patient's intentional underdosing of medication regimen due to financial hardship) • Z91128 (Patient’s intentional underdosing of medication regimen for other reason) • Z91130 (Patient’s unintentional underdosing of medication regimen due to age-related debility) • Z91138 (Patient’s unintentional underdosing of medication regimen for other reason) Shows whether or not the patient’s noncompliance was intentional, but also identifies if the patient needs some form of assistance from social services, etc.
Diagnosis Coding (ICD-10-CM)
ICD-10-CM • Allows for greater “specificity & detail” which is currently lacking in ICD-9-CM. • Moving from 14,000 ►69,000 diagnosis codes! • 25,000 (36%) of all ICD-10-CM diagnosis codes will now distinguish ‘right’ vs. ‘left’. • Must be documented in the medical record for code capture. • Expanded # of characters of the ICD-10-CM diagnosis codes will provide greater specificity to identify: etiology, anatomical site, & severity
Why Are There So Many New Codes? • Main difference between ICD-9-CM and ICD-10-CM codes, outside of structural changes, is the “SPECIFICITY” of the code. • ICD-10-CM diagnosis codes will range anywhere from 3 to 7 characters which will allow us to capture this greater detail. • But it must be documented in the record!
ICD-9-CM vs. ICD-10-CM ICD-10-CM • 3 - 7 digits or characters • 1st character is alpha (all letters used except “U”) • 2nd – 7th characters can be alpha and/or numeric • Decimal placed after the first 3 characters (the same!) • 21 Chapters and “V” & “E” codes are ‘not’supplemental • 69,000+ diagnosis codes ICD-9-CM • 3 - 5 digits or characters • 1st character is numeric oralpha (E or V codes) • 2nd – 5th characters are numeric • Decimal placed after the first 3 characters • 17 Chapters and “V” & “E” codes are ‘supplemental’ • 14,000 diagnosis codes
Level of Detail Example • ICD-9-CM (Irregular Astigmatism) (367.22) • Only 1 code in ICD-9-CM • ICD-10-CM (Irregular Astigmatism) • Will have four choices: • H52.211 (irregular astigmatism, right eye) • H52.212 (irregular astigmatism, left eye) • H52.213 (irregular astigmatism, bilateral) • H52.219 (irregular astigmatism, unspecified eye) • Physicians are likely documenting “laterality” now, but coders aren’t looking for it. • One easy place to look for documentation improvement!
Biggest Change in ICD-10-CM LATERALITY • For bilateral sites, the final character of the codes in ICD-10-CM indicate laterality. • Right side is always character 1 (RT) • Left side is always character 2 (LT) • Bilateral code is always character 3 (RT & LT) • But be careful! Not all codes will have a ‘bilateral’ distinction, i.e., carpal tunnel, etc. • “Unspecified” side code is also provided should the side not be documented in the medical record. Did we just lose our specificity?
Diagnoses That Will Require Laterality • Joint pain • Joint effusion • Injuries • Fractures • Dislocations • Arthritis • Cerebral infarction • Extremity atherosclerosis • Pressure ulcers • Cancers, neoplasms (breast, lung, bones, etc.)
Injuries • Seventh (7th) character identifies the patient encounter type, with “A” for the initial encounter, “D” for the subsequent encounter and “S” for sequelaencounter. • Initial = Patient is receiving ‘active’ treatment • First time being seen for the injury, i.e., ER visit, surgery, evaluation by new physician • Subsequent = Follow-up care • Sequela = Complication of a previous injury
Examples of ICD-10-CM Emergency Room • I10 Essential (primary) hypertension • S01.02xA Laceration with foreign body of scalp, initialencounter • S01.02xD Laceration with foreign body of scalp, subsequent encounter • S02.2xxA Fracture of nasal bones, initial encounter for closed fracture • H65.01 Acute serous otitis media, right ear • H65.02 Acute serous otitis media, left ear • H65.03 Acute serous otitis media, bilateral
Procedure Coding (ICD-10-PCS)
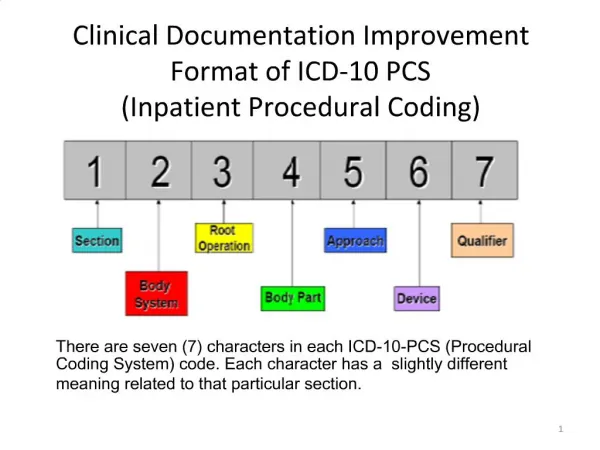
ICD-10-PCS Characters (Medical and Surgical Section) Root SectionOperationApproachQualifier BodyBodyDevice System Part
Dissect ICD-10-PCS Code Endoscopic Esophageal Excision via Natural or Artificial Opening ICD-9-CM: 45.16 Esophagogastroduodenoscopy (EGD) with Closed Biopsy
Obstetrics • Under ICD-10-CM diagnosis codes will be based on the stage of pregnancy • First trimester • Second trimester • Third trimester • Trimesters are counted from the first day of the last menstrual period, and defined as: • First trimester: Fewer than 14 weeks • Second trimester: Fourteen weeks • Third trimester: Twenty-eight weeks
Nicotine Dependence • ICD-10-CM contains a separate category for nicotine dependence with subcategories to identify the specific tobacco productand nicotine-induced disorder(s). For example: • Cigarettes • Chewing tobacco • Cigar, etc. • ICD-9 has only one diagnosis code (305.1) for tobacco use disorder or tobacco dependence.
Underdosing • New diagnosis code in the ICD-10 world! • Identifies situations in which a patient has taken less of a medication than prescribed by the physician and captures those reason(s). • Must be documented in the record! • Financial • Non-compliance*
Burns and Corrosions • Burn codes identify: • Thermal burns, except for sunburns, that come from a heat source • Burns resulting from electricity and/or radiation • Addition of the term “corrosion” is new in ICD-10-CM: • Corrosions are burns due to chemicals
Top 10 Documentation ‘Pearls’ • Laterality (left vs. right) • Stage of Care (initial or follow-up) • Specific Diagnosis (acute vs. chronic) • Specific Anatomy (specific bone in the hand) • Associated and/or Related Conditions • Cause of Injury (hit by baseball, fall) • Documentation of Additional Symptoms or Conditions • Dominant vs. Non-Dominant Side • Tobacco Exposure or Use • Gustilo-Anderson Scale
Documentation Tips For Specific Diagnoses
GERD Documentation • ICD-10-CM will include 2 codes but does not include the abbreviation “GERD” • K21.0 (Gastro-esophageal reflux disease with esophagitis) • K21.9 (Gastro-esophageal reflux disease without esophagitis) • Barrett’s now broken down: • With or without ulcer • With or without dysplasia • Staging of dysplasia • Low grade • High grade
Digestive Ulcer • Documentation needs to include the specific location: • Gastric • Duodenal • Peptic • Gastrojejunal • Further specificity needs to identify: • Acute or chronic • With hemorrhage • With perforation • With hemorrhage and perforation • Without mention of hemorrhage or perforation
Asthma Documentation • Document the Severity (3 levels): • Mild(more than two times per week) • Moderate (daily and may restrict physical activity) • Severe (throughout the day with frequent severe attacks limiting the ability to breathe) • Clarify whether acute, chronic, intrinsic or extrinsic • Specify exercise-induced or other forms • Specify when chronic state asthmatic bronchitis exists and when acute exacerbation occurs • Document tobacco exposure or history of
Congestive Heart Failure • Documentation in ICD-10-CM needs to identify whether the CHF is acute or chronic and the specific ‘type’ of heart failure: • Combined systolic & diastolic • Diastolic • Systolic • Left ventricular
Bronchitis • Need to include specificity such as: • Acute or subacute • Further specify with bronchiectasis, COPD, etc. • Allergic • Asthmatic • Chronic • Obstructive • Viral
Diabetes Mellitus • ICD-9 features 59 codes for diabetes, while ICD-10 offers more than 200 and adds a provision of “poorly controlled” to categories of controlled or not controlled. • Diabetes mellitus codes expanded to include the classification of the diabetes AND the manifestation. • Needs to be clearly documented in the record!
More on Diabetes • Identify Type 1, Type 2, due to other secondary cause, i.e., gestational, etc. • In Type 2 or secondary cause, identify when using insulin long-term • Identify all body systems affected by the diabetes (neuropathy and its manifestation, retinopathy and proliferative or nonproliferative, nephropathy and stage of CKD, vasculopathy, etc.) • Identify all manifestations (ulcer, coma, gangrene, osteomyelitis, etc.)
Hypertension & CKD • When a patient has both a diagnosis of hypertension and CKD, there is an assumed ‘cause and effect’ relationship and will be reported as “hypertensive chronic kidney disease, stage I through stage IV, or unspecified, unspecified benign or malignant”. • If not related, provider documentation must be stated as not due to hypertension.
Additional documentation needs to include: • Stage I • Stage II (mild) • Stage III (moderate) • Stage IV (severe) • Stage V • Requiring chronic dialysis • End-stage renal disease
Chest Pain • Medical record documentation must include the specific location of the chest pain: • Anterior wall • Atypical • Intercostal • Musculoskeletal • Non-cardiac • Precordial
Fracture Documentation • Documentation will need to include the following to accurately code a fracture in ICD-10-CM: • Displaced or non-displaced • Open or closed • Laterality (left vs. right vs. bilateral) • Specific bone and location of the bone • Distal, proximal, mid-shaft, etc. • Encounter • Initial, subsequent, sequela
Fracture “Subsequent” Encounter • Subsequent encounter for open and closed fractures: • Used for encounters afteractive fracture treatment has been completed and the patient is receiving routine care during the healing or recovery period. • Closed Fracture 7th Character Extensions: • D ► Routine healing or aftercare • G ► Delayed healing • K ► Nonunion • P ► Malunion
What is Gustilo-Anderson Scale? • Gustilo-Anderson classification identifies the ‘severityof soft tissue damage’ in open fractures – may be new to coders and physicians: • Type I: Wound is smaller than 1 cm, clean, and generally caused by a fracture fragment that pierces the skin (low energy injury) • Type II: Wound is longer than 1 cm, not contaminated, and w/o major soft tissue damage or defect (low energy injury) • Type III: Wound is longer than 1 cm, with significant soft tissue disruption. The mechanism often involves high-energy trauma, resulting in a severely unstable fracture with varying degrees of fragmentation.
Hernias • Specify location (inguinal, femoral, umbilical, ventral, diaphragmatic; all other abdominal hernias default to “other”, etc.) • Specify unilateral (which side) or bilateral • Specify with obstruction when present • Specify with gangrene when present • Specify when recurrent hernia (defaults to primary)
Malignancy Example • Malignant Neoplasm Lung/Bronchus • 63 choices available in ICD-10-CM • Documentation must include: • Specific site/location: • Hilus, lingula, main bronchus, lower lobe, middle lobe, upper lobe, etc. • Laterality • Tobacco exposure or use (secondary diagnosis) • Example: C34.2 (Malignant neoplasm of middle lobe, bronchus or lung)
Physician Practices • ICD-10-CM diagnosis codes will impact every physician practice large or small! • Look at all areas that will impact your practice and identify each one that will be affected: • Practice Management System • Electronic Medical Record (EMR) • Paper record • Superbill/encounter form – Does it have diagnosis codes on it? • Lab requisitions
Task Is Not As Huge As It Appears! • Although the coding book is “huge”, many physician practices use only a small set or # of diagnosis codes. • Start developing crosswalks between ICD-9-CM & ICD-10-CM codes you use most frequently in the office. • Revise your superbill/encounter form if it currently contains ICD-9-CM codes.
Contact Info: Karen Kvarfordt, RHIA, CCS-P, CCDS AHIMA Certified ICD-10 Trainer President, DiagnosisPlus, Inc. PO Box 486 Pocatello, ID 83204 (208) 221-5486 diagnosisplus1@live.com