Download
1 / 35
360 likes | 976 Views
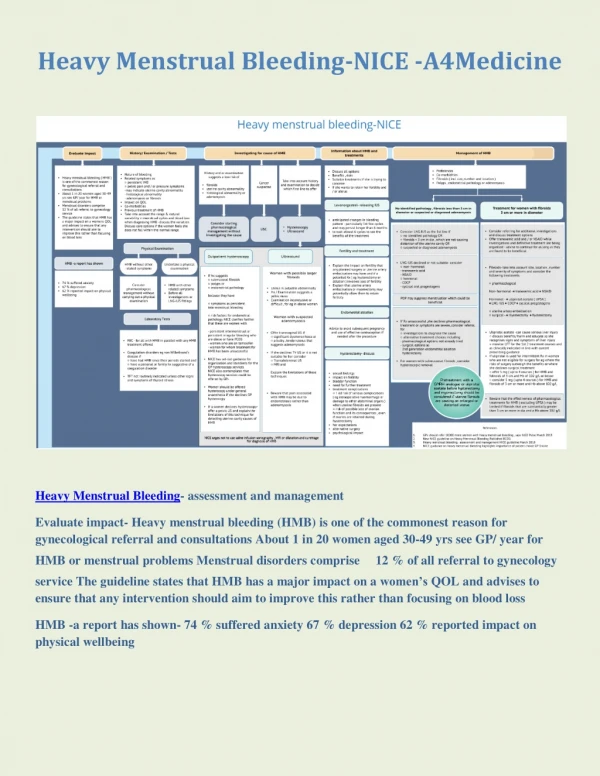
Cyclic Heavy Menstrual Bleeding. David Hilmers , M.D. MLK Clinic Lecture. Objectives. Explain the role that hemostatic mechanism play in cyclic heavy menstrual bleeding (HMB)

E N D
Cyclic Heavy Menstrual Bleeding David Hilmers, M.D. MLK Clinic Lecture
Objectives • Explain the role that hemostatic mechanism play in cyclic heavy menstrual bleeding (HMB) • Describe the risks and benefits of options for managing cyclic HMB, with a focus on nonsurgical, noncontraceptive therapy • Incorporate evidence-based treatment into clinical practice • Provide individualized counseling to help patients choose customized optimal treatment plans
Consequences of HMB • Associated with increased health care utilization • Lost work estimated at $1692 annually (in 1999) • May cause discomfort, anxiety, and impaired quality of life
Characteristics of Normal Menstrual Cycles • Cycle length: 21-35 days • Bleeding duration: < or = 7 days • Average blood loss: 35 ml (range 20-60 ml)
Cyclic HMB defined • Excessive or prolonged (> 7 days) uterine bleeding occurring at regular intervals, every 21-35 days • Clinically defined as menstrual blood loss (MBL) > or = 80 ml per cycle • Also referred to as hypermenorrhea or menorrhagia
Causes of HMB Organic (organ Dysfunction, bleeding disorders Endocrine Anatomic (fibroids) Iatrogenic (IUD, Chemo, anticoags) Thyroid disorders Pituitary tumors Clinical Causes of HMB
Causes of Cyclic HMB: Hemostatic disorders • Systemic hemostatic disorders -Inherited coagulation disorders -Acquired disorders -Iatrogenic • Local hemostatic disorder -Endometrial hemostatic dysfunction
Causes of Cyclic HMB: Systemic Hemostatic Disorders • Inherited coagulation disorders -von Willebrand disease -Hemophilias • Acquired disorders -ITP/TTP -Liver disease -Leukemia • Iatrogenic -Anticoagulants -NSAIDs
Von Willebrand’s Disease • Most common inherited bleeding disorder—AD with variable penetrance • Seen in 1/3 of adolescents with HMB • Symptoms: easy bruising, excessive bleeding after procedures, nose bleeds, HMB
Age, parity Cyclic vs. noncyclic bleeding Singular vs. chronic episodes Duration and amount of bleeding Significance/impact Contraceptive method Marital status/sexual history History of bleeding disorders Medical illnesses Medications Family history Evaluation of Abnormal Bleeding History
Diagnosis of Cyclic HMB • Subjective -Patient perception -Patient history • Objective—NOT required for diagnosis -Examination during heaviest flow -Completed menstrual calendar -Anemia
Evaluation of Cyclic HMB: Lab • CBC, platelet count • Pap smear (only if indicated, i.e., if patient is due) • Coagulation studies should be considered if: -HMB since menarche -Hx of bleeding (postpartum, surgery, dental, bruising, epistaxis, gum bleeding) -Family history of bleeding symptoms
Evaluation of Cyclic HMB: Procedures and Imaging -Endometrial biopsy—if at risk for endometrial hyperplasia -Transvaginal U/S – if pelvic exam is inadequate or findings are abnormal
Medical Management of Cyclic HMB • Off-label therapies -NSAIDs -OCP’s -Depot Provera • FDA-approved therapies -Hormonal: Progestins -Nonhormonal: Tranexamic acid
NSAIDs: Off-label Use • Several studies show reduction in blood loss compared to placebo • Initiated immediately before or on first day of menses for up to 5 days • Less effective than other medical modalities • Approximately 20% decrease in blood loss • No evidence of differences among NSAIDs
Combination OCPs Off–label use • Often used off label for HMB, despite limited data -Continuous OCP use may be superior to standard regimen -For break-through bleeding with continuous OCPs, stop 3 days and then restart (>90% resolution in bleeding) • Recent study compared phasic OCP (E2 valerate/dienogest) to placebo -Approximately 70% reduction in mean blood loss in OCP group -19% reduction in placebo group -Regimen approved for treatment of HMB in Europe
DMPA: Off-label use • Dose: 150-250 mg IM q 2-3 months -FDA-approved for contraception only (150 mg q 3 mos) -Disadvantages: -High incidence of irregular bleeding -Bone loss with long-term use -Weight gain
FDA-Approved Therapies • Hormonal: Progestins • Nonhormonal: Tranexamic acid
Oral progestins • In a randomized trial of women with HMB, low dose medroxyprogesterone (MPA) 10 mg x 10 days (beginning on cycle day 16) reduced blood loss by only 21.5% at 6 months (Kaunitz AM, et al. Obstet Gynecol. 2010.116:625-632._ • In another study, norethindrone 6 mg tid on cycle days 5-26 reduced bleeding by 87% after 3 cycles -Only 22% wished to continue treatment (Irvine GA, et al. Br J Obstet Gynecol 1998. 105:592-98)
Levonorgestrel IUD • Recommended for women who have had a child • Indicated to treat HMB in women who choose to use IUD as their method of contraception • Use off label in women who do not require contraception
Changes before and after IUD insertion Xiao. Treatment of menorrhagia with LNG-IUS. Fertil Steril 2003.
Levonorgestrel IUD vs. Hysterectomy for HMB • 5 year study • 236 Women were randomized -Levonorgestrel (LNG) IUD (n=119) and hysterectomy (n=117) -58% of the LNG IUD group did not require subsequent hysterectomy • Quality of life benefits were equal in both groups -Costs were lower in the LNG IUD group -Satisfaction with treatment similar between groups
Medical Mgt of HMB – Tranexamic Acid • Approved by the FDA 2009 to treat cyclic HMB -Long history of use for HMB in other countries • Mechanism of action: synthetic lysine amino acid derivative; diminishes the dissolution of hemostatic fibrin by plasmin, stabilizing fibrin matrix (antifibrinolysis) • Concern about thromboembolic events not substantiated in recent studies
Tranexamic Acid • Only FDA-approved nonhormonal therapy of cyclic HMB • Dose: Two 650-mg tabs 3 times/day for a maximum of 5 days during menstruation • Contradindicated if history of or increased risk for venous thromboemboloism • Use with OCPs may increase risks of arterial/venous thrombosis
MBL with tranexamic acid vs placebo Lukes A, et al. Obstet Gyn. 2010.116(4):865-875
Medical Management of Cyclic HMB: Factors to Consider • Need for contraception • Patient preference: may desire to avoid hormones, devices, or surgery • Contraindications to hormonal therapies • Size of uterus; presence, size, and location of fibroids • Cost • Compliance • Social/cultural considerations
Case 1: Susan. Avoiding Surgery, Hormones • 33 yo G3P3 with monthly HMB, anemia • Was offered surgery (ablation/hysterectomy, but is wary; seeking a second opinion) • Strong family history of breast cancer (mother and sister); wants to avoid hormone use • Husband has had a vasectomy • No history of surgery, illness, normal pelvic exam
Options • What would be the most appropriate option for her to consider? • She should proceed with surgical management • Medroxyprogesterone acetate • Tranexamic acid • Levonorgestrel IUD
Case 2: Celeste. A smoker with no need for contraception • 35 yo G2P2 with monthly HMB • Does not want to be pregnant at this time • History of acne treated with isotretinoin • Smokes half a pack per day • Hx/PEX otherwise unremarkable
Celeste • What is best option • She should proceed with surgical management • Medroxyprogesterone acetate • Tranexamic acid • Levonorgestrel IUD
Case 3: Celia • 20 yo G0P0 complains of HMB • Not sexually active currently or in the bpast, but is dating the same man for the past 6 months • No other menstrual problems or complaints • PMHx: Unremarkable • PEX: Normal
Would you advise Celia to consider… • OCPs. She can use contraception even if she isn’t currently sexually active. • Levonorgestrel IUS; effective treatment for pregnancy prevention and HMB. • Tranexamic acid. It is highly effective for the treatment of HMB, but does not provide contraception. • NSAIDs. Efficacy is not optimal, but they are readily available OTC and may provide some benefit. • All of the above.
Hemostatic disorders • Systemic hemostatic disorders can be either inherited, acquired or iatrogenic. Which of the following inherited disorders is the most common in adolescents with HMB? • ITP / TTP • Von Willebrand's Disease • Hemophilia • Endometrial hemostatic dysfunction
Conclusions • Cyclic HMB is common and disruptive to life of many women • --Most cyclic HMB can be medically managed • --Several progestin dominant formulations are available for management • --An FDA-approved nonhormonal option is now available