Download
1 / 47
560 likes | 1.21k Views
BRAIN ABSCESS. M.RASOOLINEJAD, MD DEPATMENT OF INFECTIOUS DISEASE TEHRAN UNIVERSITY OF MEDICAL SCIENCE. BRAIN ABSCESS. Focal & Suppurative Process in Brain Parenchyma. Anatomical Relationships of the Meninges. Bone Dura Mater Arachnoid Pia Mater Brain.

E N D
BRAIN ABSCESS M.RASOOLINEJAD, MD DEPATMENT OF INFECTIOUS DISEASE TEHRAN UNIVERSITY OF MEDICAL SCIENCE
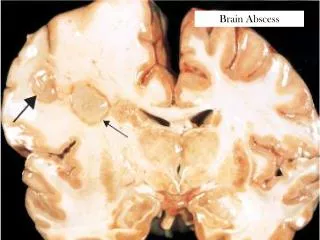
BRAIN ABSCESS Focal & Suppurative Process in Brain Parenchyma
Anatomical Relationships of the Meninges • Bone • Dura Mater • Arachnoid • Pia Mater • Brain • Epidural Abscess • Subdural Empyema • Meningitis
EPIDEMIOLOGY • Uncommon intracranial infections • Incidence 1:100,000/year • Predisposing conditions: Paranasal Sinusitis • Otitis Media • Dental infections • Immunocompromised pts Uncommon org • (T.gondii, Aspergillus spp, Nocardia spp, …)
ETHIOLOGY • Abrain abscess may develop: • Direct spread from a contagious cranial of infections • ( Paranasal sinusitis, Otitis media, Mastoiditis,…..) • 2. Following head trauma or Neurological procedure • 3. Hematogenous spread from remote site of inf • 4. No obivious primary source of inf ( 20-30% ) • (Cryptogenic brain abscess )
ETHIOLOGY • Most common organisms are : • Paranasal sinusitis:Microaerophilic & • Anaerobic strep • Haemophilus spp • Bacteroides spp • Fusobacterium spp • Dental infections: Streptococci spp • Prevetella • Prophyromanas
ETHIOLOGY Most common organisms are : Otitis media & Mastoiditis: Streptococci Bacteroides spp P. aeroginosa Enterobacteriaceae Hematogenous: S. Viridance S. Aureous Neurosergical procedure & open head trauma: (S. aureous, Enterobactericeae, P. aeroginosa)
SOURSE OF BRAIN ABSCESS • Frontal lobe:Frontal & Ethmoidal & Sphenoidal sinuses • Dental infections • Temporal lobe: Middle ear, Mastoid, Maxillary sinuses • Cerebellum & Brain Stem: Middle ear & Mastoid • Posterior Frontal or Parietal lobes: • Middle Cerebral Artery • Gray- White matter • Often multiple
PATHGENESIS • Bacterial invasion of brain • (Parenchyma ) • Preexisting or concomitant : • Ischemia & • Necrosis & • Hypoxia of brain tissue
PATHGENESIS 4 Stages Brain Abscess formation: Stage 1 • Early cerebritis ( days 1 to 3 ) • Prevascular infiltration of inflammatory cells • Central core of coagulative necrosis • Marked edema surrounds the lesions
PATHGENESIS 4 Stages Brain Abscess formation: Stage 2 • Late cerebritis ( days 4 to 9 ) • Pus formation ( necrotic center ) • Macrophages & Fibroblastrs • Thin capsule ( Fibroblast & Reticular fibers ) • Marked edema around the lesions
PATHGENESIS 4 Stages Brain Abscess formation: Stage 3 • Early Capsule formation ( days 10 to13 ) • Capsule formation • Ring-enhancing capsule ( Imaging )
PATHGENESIS 4 Stages Brain Abscess formation: Stage 4 • Late Capsule formation ( > 14 days ) • Well formed necrotic center • Dense peripheral collagenous capsule • No cerebral edema • Marked gliosis & reactive astrocytes • Gliosis Seizures
CLINICAL PRESENTATIONS Brain abscess presents as an Expanding Intracranial mass • Headache > 75% • Constant, Dull, • Aching sensation • Hemicranial or General • Progressive Refractory • Fever: 50% & Low grade • Seizure: New onset • Focal or Generalized
CLINICAL PRESENTATIONS • Increased Intracranial Pressure: • Papilledema • Nausea • Vomiting • Drowsiness • Confusion • Meningismus: • When it has ruptured into Ventricle or subarachnoid space
CLINICAL PRESENTATIONS • Focal neurologic deficit > 60% • Frontal lobe Hemiparesis • Mental status, Drowsiness • Temporal lobe Dysphasia Upper homonymous quadrantanopia Ipsilateral headache
CLINICAL PRESENTATIONS • Focal neurologic deficit > 60% • Cerebellar Nystagmus, Ataxia • Dysmetria, vomiting • Brain stem Facial weakness, • Fever, Hemiparesis, Dysphagia, • Vomiting, Headache, Fever
DIAGNOSIS NEUROIMAGING STUDIES • Brain CT- Scan • MRI ( Early cerebritis, Posterior Fossa) • Steriotactic Needle aspiration • Lumbar puncture Risk of Herniation • CSF Non Specific • Peripheral leucocytosis: 50% • Elevated ESR: 60%
TREATMENT SURGICOMEDICAL • Aspiration Or Open Drainage • Empirical Combination • Antimicrobial Therapy • Duration: 6 to 8 wks IV • Prophylactic Anticonvulsant Therapy • Glucocorticoids( Severe Edema & ICP ) • Serial CT-Scan or MRI
ANTIMICROBIAL THERAPY • Otitis media & Mastoiditis: • Metronodazole & 3rd Cephalosporin • Sinusitis: • Metronidazole & 3rd Cephalosporine • Dental Sepsis: • Penicillin & Metronidazole
ANTIMICROBIAL THERAPY • Penetrating trauma &Neurosurgury: • Vancomycin & 3rd Cephalosporin • Bacterial endocarditis: • Vancomycin & Gentamycin • Nafcilline (Oxacillin) & Ampicillin • & Gentamycin • Unknown: • Vancomycin & Metronidazole & 3rd Cephalosporin
PROGNOSIS • Successfully treatment • Good prognosis • Seizures are a • common complication 70%
THE END