Download
1 / 34
350 likes | 522 Views
H + secretion (proximal tubule/thick ascending Henle). Proximal tubule (~80%), thick ascending limb (~15%) of H + secreted. Mechanisms of H + secretion ( intercalated cell). intercalated cell (~5% of H + secreted). Bicarbonate reabsorption & synthesis.

E N D
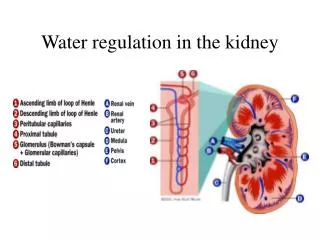
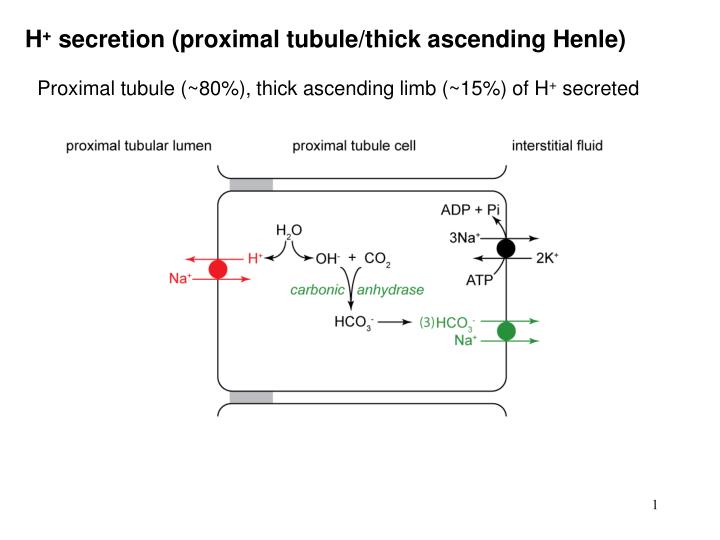
H+ secretion (proximal tubule/thick ascending Henle) Proximal tubule (~80%), thick ascending limb (~15%) of H+ secreted
Mechanisms of H+ secretion ( intercalated cell) intercalated cell (~5% of H+ secreted)
Bicarbonate reabsorption & synthesis if no HCO3- production or utilization: recycled HCO3- would ensure HCO3- balance if HCO3- used for buffering: new HCO3- replaces it
Quantitation of secreted H+ & reabsorbed HCO3- “Titratable acidity” = excreted H2PO4-& other urinary buffers “Urinary ammonium” = excreted NH4+
Important principles 1 H+ secreted = HCO3-reabsorbed H+ excreted = titratable acidity + urinary NH4+ Most of the H+ secreted is used to “reclaim” filtered HCO3- Filtered HCO3- is not reabsorbed as such; it is destroyed in tubule and resynthesized in tubular cell New HCO3-synthesized = H+ excreted = titratable acidity + urinary NH4+
Important principles 2 Plasma [HCO3-] depends on the rate of renal H+secretion H+secretion plasma [HCO3-] (metabolic alkalosis) H+secretion plasma [HCO3-] (metabolic acidosis) Healthy kidney maintains the constancy of plasma [HCO3-] by maintaining constancy of H+secretion (irrespective of moderate acid or alkaline assaults)
Henderson Hasselbalch equation H2O + CO2 H2CO3H+ + HCO3- Looking at 2nd half of equation: K (equilibrium constant) = [H+] x [HCO3-] [H2CO3] Rearranging and taking negative logs: pH = pK + log10 [HCO3-] [H2CO3] Assuming the 1st half of the equation is at equilibrium: [H2CO3] = 0.03 x Pa.CO2 Then, the Henderson Hasselbalch equation is: pH = pK + log10 [HCO3-] 0.03 x Pa.CO2
Why use the bicarbonate buffer system? Not ideal because: pK 6.1, and buffers are most effective around their pKs However: the body can regulate Pa.CO2 & [HCO3-] independently and thus control pH lungs regulate Pa.CO2 & kidneys regulate [HCO3-] regulating pH will alter all buffer systems (isohydric principle) clinically, we can measure pH & Pa.CO2, & calculate [HCO3-]
Interpreting acid base data (DRW AIM) Normal values: pH 7.35 – 7.45, Pa.CO2 33 – 44 mm Hg, HCO3- 22 – 28 mEq/L 1. Acidosis or alkalosis? pH < 7.35 = acidosis, pH > 7.45 = alkalosis you may have to revise that later, but start with this “overcompensation” does not occur
Metabolic or respiratory? 2a. Is it metabolic acidosis (alkalosis)? Look at [HCO3-]; metabolic alkalosis, metabolic acidosis e.g. pH 7.25, [HCO3-] 14 mEq/L = Yes; metabolic acidosis e.g. pH 7.25, [HCO3-] 32 mEq/L = No; not metabolic acidosis 2b. Is it respiratory acidosis (alkalosis)? Look at Pa.CO2; respiratory acidosis, respiratory alkalosis e.g. pH 7.25, Pa.CO2 64 mm Hg = Yes; respiratory acidosis e.g. pH 7.25, Pa.CO2 26 mm Hg = No; not respiratory acidosis
Respiratory compensation 3. Respiratory compensation (metabolic disorders) Mechanism: pH or pH detected by carotid body & aortic arch chemoreceptors, ventilation rate Pa.CO2; ventilation rate Pa.CO2 Features: rapid response (minutes); no response suggests respiratory disorder relatively inadequate because Pa.CO2 limits response i.e. metabolic acidosis AVR Pa.CO2 AVR Pa.CO2 > 55 mm Hg is respiratory acidosis (too high for compensation)
Metabolic compensation 3. Metabolic compensation (respiratory disorders) Mechanism: Pa.CO2 or Pa.CO2 causes or H+ secretion & HCO3- reabsorption Features: buffering is not compensation [HCO3-] will by ~1 mEq/L for each 10 mm Hg Pa.CO2 (buffering) slow response ~ 24 hrs for [HCO3-] (excretion) days for [HCO3-] (induction of glutaminase II) very effective (eventually)
Terminology (compensation vs. mixed condition) pH 7.30, [HCO3-] 14 mEq/L, Pa.CO2 29 mm Hg is compensated metabolic acidosis, not (mixed) metabolic acidosis and respiratory alkalosis pH 7.34, [HCO3-] 32 mEq/L, Pa.CO2 62 mm Hg is compensated respiratory acidosis, not (mixed) respiratory acidosis and metabolic alkalosis Compensation will disappear when the primary condition is treated; a mixed condition won’t
Anion gap; why does it change? The “gap” is [measured cations] - [measured anions]
Significance of the anion gap Used for differential diagnosis of metabolic acidosis Hyperchloremic metabolic acidosis (normal anion gap) occurs when disorder is HCO3- loss, e.g. diarrhea, renal tubular acidosis, carbonic anhydrase inhibitors, Addison’s disease Normochloremic metabolic acidosis (increased anion gap) occurs when “non HCl” acids accumulate e.g. lactic acidosis, ketoacidosis, salicylate, methanol (formate), ethylene glycol (glycolate, oxalate), chronic renal failure (sulfate, phosphate, others)
Causes of respiratory acid base disorders Respiratory acidosis: opiates, sleep apnea, administration of O2 to a “blue bloater” type of COPD, weakness of respiratory muscles, extreme obesity, pulmonary edema, asthma, pneumonia, pneumothorax Respiratory alkalosis: several respiratory diseases (pneumonia, interstitial fibrosis, pulmonary embolus), hyperventilation, liver failure, salicylate overdose, gram negative septicemia, mechanical ventilation
Causes of metabolic acid base disorders Metabolic acidosis (hyperchloremic, normal anion gap): diarrhea, carbonic anhydrase inhibitors, aldosterone deficiency, types I & II renal tubular acidosis Metabolic acidosis (normochloremic, increased anion gap): diabetic ketoacidosis, lactic acidosis, chronic renal failure, various poisonings (salicylate, methanol, ethylene glycol) Metabolic alkalosis: antacid ingestion, vomiting, nasogastric suction, loop or thiazide diuretics, aldosterone excess, vascular volume depletion, potassium depletion
Case F1: acid base condition pH 7.58; Pa.CO2 23 mm Hg; [HCO3-] 21 mEq/L 1. Look at pH (is it acidosis or alkalosis?) pH = 7.58 alkalosis 2. Look at HCO3- (is it metabolic alkalosis?) HCO3- = 21 mEq/L (normal 22-30) not metabolic alkalosis 3. Look at Pa.CO2 (is it respiratory alkalosis?) Pa.CO2 = 23 mmHg (normal 35-45) respiratory alkalosis • See if appropriate compensation has occurred: compensation for respiratory alkalosis is HCO3- excretion HCO3- = 21 mmHg (normal 22-30) uncompensated i.e. acute respiratory alkalosis
Case F1: questions Describe her acid base condition acute respiratory alkalosis Plausible causes for her acid base condition? hysterical hyperventilation Suggest causes of her dizziness Pa.CO2 cerebral vasoconstriction Any evidence for ventilation/perfusion mismatch in pulmonary function? A-a O2 difference = 123-116 = 7 (i.e. OK) What is carpopedal spasm, and its possible cause? pH Ca++ binding to albumin free [Ca++] more negative threshold for muscle cell depolarization (Na+ channel sensitivity) hypocalcemic tetany
Case F2: acid base condition pH 7.29; Pa.CO2 26 mm Hg; [HCO3-] 12 mEq/L 1. Look at pH (is it acidosis or alkalosis?) pH = 7.29 acidosis 2. Look at HCO3- (is it metabolic acidosis?) HCO3- = 12 mEq/L (normal 22-30) metabolic acidosis 3. Look at Pa.CO2 (is it respiratory acidosis?) Pa.CO2 = 26 mmHg (normal 35-45) not resp. acidosis • See if appropriate compensation has occurred: compensation for metabolic acidosis is hyperventilation Pa.CO2 = 26 mmHg (normal 35-45); partial compensation 5. Anion gap = 142 - (100 + 12) = 30 (increased) i.e. partially compensated normochloremic metabolic acidosis
Case F2: questions Total CO2 (CO2 content)? CO2 released when venous plasma is acidified equals [HCO3-] + 0.03 x P.CO2 (units mEq/L) Describe his acid base condition partially compensated normochloremic metabolic acidosis (increased anion gap) Plausible causes for his acid base condition? normochloremic metabolic acidosis diabetic ketoacidosis: [glucose] 650 mg/dL alcoholic ketoacidosis: starvation, GNG, lipolysis lactic acidosis: bp hypoperfusion Anion gap? ketoacids (diabetes, alcohol), lactate (shock, hypoxemia)
Case F2: questions What precautions with his therapy? Aims:volume repletion, insulin, pH correction HCO3-, insulin & osmolality causes K+ to enter cells (next slide) give supplemental intravenous K+
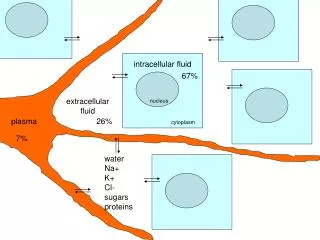
Regulation of K+ distribution Normally, 98% of total body K+ is intracellular
Case F3: acid base condition pH 7.05; Pa.CO2 45 mm Hg; [HCO3-] 12 mEq/L 1. Look at pH (is it acidosis or alkalosis?) pH = 7.05 acidosis 2. Look at HCO3- (is it metabolic acidosis?) HCO3- = 12 mEq/L (normal 22-30) metabolic acidosis 3. Look at Pa.CO2 (is it respiratory acidosis?) Pa.CO2 = 45 mmHg (normal 35-45) poss. resp. acidosis • See if appropriate compensation has occurred: compensation for metabolic acidosis is hyperventilation Pa.CO2 = 45 mmHg (normal 35-45) respiratory acidosis 5. Anion gap = 140 - (116 + 12) = 12 (unchanged) i.e. mixed hyperchloremic metabolic acidosis (normal anion gap) and respiratory acidosis
Case F3: questions 1 Describe her original acid base condition mixed hyperchloremic metabolic acidosis and respiratory acidosis Plausible causes for her acid base conditions hyperchloremic metabolic acidosis possibilities include: diarrhea, carbonic anhydrase (CA) inhibitors, aldosterone deficiency, & renal tubular acidosis (types I & II) aldosterone deficiency would have [K+], hers is 1.4 mEq/L; history rules out diarrhea, CA inhibitors, RTA, urine pH 7.0 type 1 respiratory acidosis: hypokalemia (1.4 mEq/L) decreases excitability of diaphragm
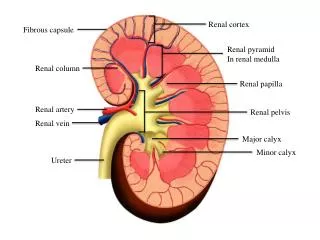
Renal tubular acidosis In general: proximal/thick ascending limb Na+/H+ exchager function is to destroy (& reabsorb) filtered HCO3- intercalated H+ ATPase is to acidify urine urinary NH4+ & titratable acidity thus synthesizing new HCO3- Proximal RTA (type 2) activity of proximal/thick AL Na+/H+ exchanger serum [HCO3-] proximal HCO3- load; serum [HCO3-] stabilizes collecting duct H+ ATPase can acidify urine & synthesize “new” HCO3- urine pH within normal range Distal RTA (type 1) activity of collecting duct H+ ATPase,or back diffusion of H+ inability of synthesize “new” HCO3- by acidifying urine progressive depletion of serum [HCO3-] urine pH at alkaline end of range although body pH
Case F3: questions 2 Urine pH towards alkaline end of range (pH 4.5-7.5)? type 1 RTA is failure of collecting duct H+ secretion (acidifying region; generating new HCO3-) Increased [HCO3-] in emergency room ( = +13 mEq/L)? buffering (1 mEq/L per 10 mm Hg Pa.CO2); Pa.CO2 = +94 mm Hg, i.e. ~10 mEq/L [HCO3-] Role of hypokalemia? hyperpolarization muscle weakness (diaphragm)
Case F3: questions 3 Cause of hypokalemia (1.4 mEq/L)? “Holy Grail” of collecting duct function (Na+ for K+ and/or H+) next slide Urinary NH4+ & titratable acidity? failure to acidify urine & synthesize “new” HCO3- Kroger’s chemical? daily NaHCO3 (baking soda) would work she was given polycitra-K (K citrate & citric acid) citrate metabolized as citric acid, removing H+ then, OH- + CO2 HCO3-
Case F4: acid base condition pH 7.44; Pa.CO2 65 mm Hg: [HCO3-] 43 mEq/L 1. Look at pH (is it acidosis or alkalosis?) pH = 7.44 it’s close, but on alkalotic side of normal 2. Look at HCO3- (is it metabolic alkalosis?) HCO3- = 43 mEq/L (normal 22-30) metabolic alkalosis 3. Look at Pa.CO2 (is it respiratory alkalosis?) Pa.CO2 = 65 mmHg (normal 35-45) not resp. alkalosis • See if appropriate compensation has occurred: compensation for metabolic alkalosis would be hypoventilation Pa.CO2 yes, but Pa.CO2 too high for compensation respiratory acidosis i.e. mixed metabolic alkalosis and respiratory acidosis
Case F4: questions Describe his acid base condition mixed metabolic alkalosis and respiratory acidosis Plausible causes for his acid base condition? metabolic alkalosis: diuretic excess, mild hypokalemia respiratory acidosis: COPD with hypoventilation (CO2 insensitivity; “blue bloater”) Ventilation perfusion mismatch? A-a O2 difference = 71-45 = 26 mm Hg (not bad for age 56 & COPD); hypoventilation & V/Q mismatch hypoxemia Cause of mild hypokalemia (3.1 mEq/L)? furosemide is K+ wasting diuretic Treatment with 100% O2? hypercapnia; removal of O2 drive