Download
1 / 40
410 likes | 645 Views
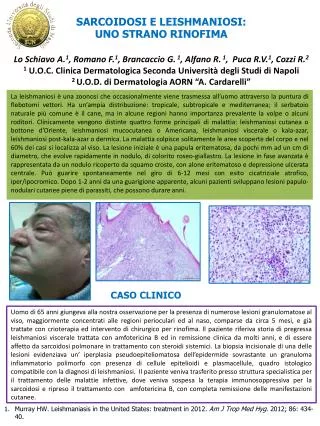
CASO CLINICO Discusso da: Dott.ssa Marika Manfrida. A.N.: 5 mesi. Giunge alla nostra osservazione per:. Grave insufficienza respiratoria in nata pretermine, con broncodisplasia e con grave ipertensione polmonare. Anamnesi familiare:.

E N D
CASO CLINICO Discusso da: Dott.ssa Marika Manfrida
A.N.: 5 mesi Giunge alla nostra osservazione per: Grave insufficienza respiratoria in nata pretermine, con broncodisplasia e con grave ipertensione polmonare. Anamnesi familiare: diabete mellito tipo II (nonno paterno e materno); ipertensione arteriosa (nonna materna e madre)
Anamnesi patologica Nata alla 27° sett di EG dopo gravidanza complicata da ritardo di crescita endouterina e gestosi al 6°mese. PN 600 gr; Indice Apgar 4-6-7 al 1’, 5’, 10’. Alla nascita somministrato Curosurf ET e posta la piccola in ventilazione meccanica in modalità SIPPV per circa un mese, è stata poi estubata e posta in NCPAP quindi respiro spontaneo con O2 in culla progressivamente ridotto fino a 0,5 L/min. A 4 mesi e mezzo peggioramento delle condizioni generali comparsa di TC febbrile e aumentato fabbisogno di O2 (PCR ed emocoltura negativa). All’ecocardio pressione polmonare 100 mmHg. Veniva avviata terapia con Sildenafil Lasix e Rocefin senza beneficio. (P polm 125 mmHg). Dopo 10 giorni per scadimento delle condizioni generali la piccola è stata reintubata e ventilata in SIPPV e trasferita da noi.
Esame obiettivo all’ingresso Peso 3,600 Condizioni generali scadute Bambina intubata e senza accesso venoso, notevolmente agitata e si oppone al respiratore. Cute pallido-grigiastra con subcianosi periorale ed al letto ungueale. Torace di forma regolare con rientramenti all’epigastrio ed agli ultimi spazi intercostali All’auscultazione penetrazione disomogenea con rantoli crepitanti diffusi. Toni cardiaci ritmici con FC 200 bpm. Addome di forma e volume regolare trattabile. Organi ipocondriaci nei limiti. Genitali esterni femminili normoconformati.
Esami all’ingresso: EGA all’ingresso: pCO2 93 mmhg, SO2 90,1 %, PO” 63,6 mmHg, pH 7,27, BE 12,4, HCO3- 36,5 Emocromo: 3500000, Hb 10,5, GB 21,2000 (N75%, E1%, L18%, M6%) PTL 256.000. PCR:1,46 Sierologia: VRS, Rosolia¸ Herpes simplex 1 e2, CMV, Toxoplasma Clamidia pneumonite, Mycoplasma pneumonite. HBV, HCV.
Esami strumentali: ETF: SI in asse VL visibili come fissurazioni. II e IV ventricolo in asse Iperecogenicità periventricolari Plessi corioidei simmetrici iperecogeni. Rx: compatibile con quadro di broncodisplasia Ecocardio: PAPs 95-100 mmHg. Ipertensione polmonare grave con PFO.
Ipertensione polmonare Condizione patologica caratterizzata dall’incremento della pressione sistolica media in arteria polmonare
CIRCOLAZIONE POLMONARE Il lume arteriolare è piccolo ed offre un’alta resistenza al flusso. Il mantenimento di alte resistenze vascolari durante la vita fetale è dovuto al rilascio di sostanze ad azione vasocostrittrice (ET-1 e leucotrieni) e bassi valori basali di vasodilatatori (ossido nitrico e PGI) o alla presenza di inibitori endogeni come l’ADMA (asymmetric dimethilarginine) che compete come substrato con l’ossido nitrico. Vita fetale: Allungamento stiramento delle cellule endoteliali; Aumento diametro vasale; Reclutamento di nuove arterie. Meccanismi passivi. Nascita Gas ematici Mediatori chimici Ossigeno Ossido nitrico vasodilatatori Meccanismi attivi Leucotrieni; Endotelina-1 (ET-1) PDGF PG CO2 Vasocostrittori Pharmacological reports, 2006, 58, suppl, 153-164.
Monitoring cardiovascular function in infants with chronic lung disease of prematurity S H Abman Arch Dis Child Fetal Neonatal Ed 2002;87:F15–F18
Manifestazioni cliniche • Cianosi • Ipossiemia refrattaria alla somministrazione di O2 anche ad alte dosi; • Tachipnea; • Ipercapnia; • Acidosi; • Epatomegalia; • Segni di insufficienza tricuspidalica.
Esami utili per la diagnosi: Laboratorio: emogasanalisi – emocromo - PCR- emocultura- funzionalità epatica e renale- coagulazione – transaminasi. Esami strumentali: Rx torace – Ecocardiogrammacolordopler – TAC torace – RMN – angiografia polmonare – biopsia polmonare
IPP: obiettivi della terapia Mantenere una PAPs < 50 mmHg Mantenere una SaO2~ 90% Mantenere una PaCO2 tra 40-60 mmHg
Strategie terapeutiche: Ventilazione meccanica: - convenzionale ad alta frequenza; - HFOV. Ipossiemia ed ipercapnia Modifica del tono vasale polmonare Vasodilatatori Terapia eziologica Terapia di supporto European Heart Journal (2004) 25, 2243–2278
IPP: Terapia DIURETICI In caso di scompenso cardiaco DOBUTAMINA In caso di depressione della contrattilità miocardica NUTRIZIONE European Heart Journal (2004) 25, 2243–2278
IPP: Terapia ANTICOAGULANTI ORALI Solo in casi selezionati ad alto rischio di trombosi per il rischio di sanguinamento acuto ANTIBIOTICOTERAPIA CARDIOCHIRURGIA European Heart Journal (2004) 25, 2243–2278
Questa figura mostra l’azione dell’ET-1 che detemina la contrazione della cellula muscolare liscia ma anche il suo rilassamento attraverso il rilasco di PGI2 e ossido nitrico (NO)
Bosentan ETB ETA Gq PIP - cAMP CONTRAZIONE IP3 - PG Silfenafil NO SMOOTH MUSCLE RELAXATION
IPP: Terapia vasoattiva Ossido Nitrico Potente vasodilatatore agisce stimolando la sintesi di cGMP con effetto miorilassante. Dose: 5-40 ppm (dose max 80 ppm) con divezzamento graduale Effetti avversi: incremento metaemoglobina, ipotensione, anomalie dell’aggregazione piastrinica. Current Pediatric Therapy
Pilot studies revealed that inhalation of NO increases systemic oxygenation in severely hypoxemic newborns with persistent pulmonary hypertension of the newborn (PPHN) [19,20]. The ability of inhaled NO to increase systemic oxygen levels was confirmed in several multicenter randomized controlled studies of term and near-term babies with hypoxemia and PH [21–23]. In one study, systemic oxygenation was observed to increase in nearly half of patients with severe PPHN who received inhaled NO [21]. Importantly, the magnitude of the increase in oxygen levels in babies treated with inhaled NO was directly proportional to the degree of hypoxia before NO inhalation, and, in 75% of the infants breathing NO, the increased systemic oxygenation was maintained over time. In another study of newborns with PPHN, the optimal concentration of inhaled NO level was investigated [24]: although the maximum increase in systemic oxygenation was observed in babies breathing 80 ppm NO, as little as 5 to 20 pm NO increased the arterial oxygen levels above those measured in babies not breathing NO. Several studies reported that, although inhaled NO did not reduce mortality in these patients, it did decrease the need for extracorporeal membrane oxygenation (ECMO), an invasive procedure that requires systemic heparinization and is not available in all intensive care nurseries [21–23]. Cardiovascular Research 75 (2007) 339–348
Inhaled NO in bronchopulmonary dysplasia Bronchopulmonary dysplasia (BPD) is a chronic lung disease of prematurely born infants that results from the inhibition or disruption of normal pulmonary alveolar and microvascular development, in part, as a result of oxygen- and ventilator-induced lung injury [25]. A number of prospective randomized controlled masked trials have now evaluated the efficacy of inhaled NO in preventing BPD and/or death in premature infants [for a comprehensive review see reference [26]]. Although an early study observed that inhaled NO did not decrease the incidence of BPD [27], a subsequent single center trial involving 207 premature infants conducted by Schrieber and colleagues suggested that inhaled NO decreases the incidence of BPD and death in prematurely born infants [28]. These latter observations were supported by data from a subsequent multicenter trial in which inhaled NO was noted to decrease the rate of BPD and death in premature infants with a birth weight N1000 g [29]. In a more recent study of 793 newborns who were 34 weeks of gestational age or less, Kinsella and colleagues reported that inhaled NO decreased the incidence of BPD in the subset of 129 infants with a birth weight of at least 1000 g [30]. Moreover, in a multicenter study of 582 premature infants with a birth weight ≤1250 g, in which inhaled NO was commenced 7 to 21 days after birth, Ballard and coworkers reported that NO inhalation improved survival without BPD [31]. Although these results are encouraging when considered together, additional studies need to be performed before the precise role of inhaled NO in preventing BPD can be defined. Cardiovascular Research 75 (2007) 339–348
IPP: Terapia vasoattiva Inibitori della fosfodiesterasi tipo 5 Silfdenafil: somministrabile per os incrementa la concentrazione intracellulare di cGMP con effetto miorilassante e antiproliferativo. Dose:0,25-2 mg/kg ogni 6 h (max 100 mg x3 vv/die). Segnalati cefalea, congestione nasale e disturbi del visus maggiori dopo 6 settimane di terapia. European Heart Journal (2004) 25, 2243–2278 Current Pediatric Therapy
Sildenafil for pulmonary hypertension in neonates Search strategy : MEDLINE, EMBASE, CINAHL databases were searched from their inception until March 2007; the Cochrane Central Register of Controlled Trials, the Cochrane Library, the reference lists of identified trials, and abstracts of meetings were searched without any language restriction. Selection criteria: Randomized or quasi-randomized controlled trials of Sildenafil compared with placebo or other pulmonary vasodilators, irrespective of dose, route and duration of administration in neonates with PPHN, were included if the trial reported any of the pre-specified outcomes. Types of participants : Both term and preterm infants (with a postnatal age of 28 days after reaching 40 weeks postmenstrual age) with primary or secondary pulmonary hypertension were included for review. Studies were included if the diagnosis was based on clinical findings with or without echocardiographic confirmation. Patients with known structural heart disease (other than patent foramen ovale or patent ductus arteriosus) were excluded. Types of intervention: The following interventions were included: 1. Sildenafil vs. placebo or no treatment 2. Sildenafil vs. another pulmonary vasodilator 3. Sildenafil and another pulmonary vasodilator vs. another pulmonary vasodilator or placebo The Cochrane Library 2008, Issue 1
Primary outcomes: 1. Hemodynamic parameters (absolute values and change from baselinemeasured after the first dose, after 24 hours, after 30 hours, after 36 hours, after 42 hours, and after the end of treatment) including: a. Pulmonary arterial pressure in mm Hg; b. Oxygenation (PaO2) or FiO2 requirement; c. Cardiac output in litre/kg/min: d. Mean arterial blood pressure in mm Hg; 2. All-cause mortality within first 28 days of life Secondary outcomes: 1. Changes in pulmonary vascular resistance index inWoods Unit m2(WUm2) (absolute values and change from baseline measured after the first dose, after 24 hours, after 30 hours, after 36 hours, after 42 hours, and after the end of treatment) 2. Changes in systemic vascular resistance index in WUm2 (absolute values and change from baseline measured after the first dose, after 24 hours, after 30 hours, after 36 hours, after 42 hours, and after the end of treatment) 3. Changes in oxygenation index (OI = PaO2 X FiO2/100) (absolute values and change from baseline measured after the first dose, after 24 hours, after 30 hours, after 36 hours, after 42 hours, and after the end of treatment) 4. Rebound increase in pulmonary arterial pressure (dichotomous) 5. Decrease in cardiac output after weaning sildenafil (dichotomous) 6. Treatment with extracorporeal membrane oxygenation (ECMO) prior to discharge 7. All-cause mortality prior to discharge 8. Length of hospitalization (days) 9. Retinopathy of prematurity (among very preterm infants < 32 weeks gestation) any stage and stage 3 or more 10. Intraventricular hemorrhage (any stage and grade 3 or more) 11. Neurodevelopmental disability at 18 - 24 months (including cerebral palsy, cognitive impairment, deafness and blindness) 12. Clinically important adverse effects reported by authors (not pre-specified) 13. Any other clinically important outcome reported by authors (not pre-specified) For all the hemodynamic parameters the change from baseline were planned to be assessed at 1, 2, 4, 6, 8, 12, 24 and 48 hours or at nearest times reported by the authors. The Cochrane Library 2008, Issue 1
A U T H O R S ’ C O N C L U S I O N S Implications for practice Safety and effectiveness of sildenafil in the treatment of PPHN has not yet been established and its use should be restricted within the context of randomized controlled trials. Implications for research Future studies are needed to evaluate safety and efficacy of sildenafil in the treatment of PPHN. The studies should be conducted both in resource limited as well as resourceful settings as different questions could be answered such as effectiveness as stand alone therapy and as an adjunct therapy. These studies will require a multicenter undertaking. Long-term neurodevelopmental follow up should be included. The Cochrane Library 2008, Issue 1
IPP: Terapia vasoattiva Antagonisti dei recettori ET-1 Bosentan: ET-2rec antagonista somministrato alla dose di: 15 mgx2 vv/die se P <10kg; 31,25 x2 se 10>P<20 kg; 62,5 mg x2 se 20>P<40; 125 mgx2 se P>40 kg Monitorizza funzionalità epatica, ematocrito ed emoglobina. Segnalato potenziale effetto teratogeno. Effetti avversi:cefalea, anemia, epatotossicità, flusng, teratonenicità.. European Heart Journal (2004) 25, 2243–2278 Clin Pharmacol Ther 2003; 73: 372-82 Current Pediatric Therapy
Response to bosentan in children with pulmonary hypertension S Maiya, A A Hislop, Y Flynn, S G Haworth Objective: To describe an early experience of treating 40 children with the dual endothelin receptor antagonist bosentan, which is known to be safe and effective in adults with pulmonary hypertension (PH). Design: In this retrospective, observational study the UK Service for Pulmonary Hypertension for children treated 40 children with bosentan, 20 with idiopathic pulmonary arterial hypertension (IPAH) (mean age 8.03 years, range 1.2–17) and 20 with PH associated with other conditions (congenital heart disease, parenchymal lung or connective tissue disease, or HIV). Their mean age was 8.3 years (range 0.6–16 years). Patients: 39 patients were in World Health Organization (WHO) class III and IV, and all had shown recent deterioration. In IPAH the mean pulmonary vascular resistance (PVR) was 21.7 units?m2 (range 5.6–42.8). In secondary PH the mean PVR was 18 units?m2 (range 4.9–49). No child had a positive response to vasodilator testing with nitric oxide. Interventions: Bosentan was given as first line treatment to 25. Nine were given intravenous epoprostenol. Children were treated for a mean of 12.7 months (range 2–24 months). Main outcome measures: Response to treatment was judged by WHO functional class, six minute walk test, weight, ECG and echocardiographic findings, and need to add additional treatment. Results: Bosentan was well tolerated. In the IPAH group 19 (95%) stabilised with bosentan treatment but 12 (60%) patients needed combined treatment with epoprostenol. In secondary PH, WHO class, six minute walk test, and weight gain improved significantly. Conclusion:Bosentan helped stabilise children with IPAH but intravenous epoprostenol was also needed by 60%. Children with secondary PH improved. Heart 2006;92:664–670.
IPP: Terapia vasoattiva Bloccanti i canali del calcio I più utilizzati sono: - nifedipina alla dose di 0,5-2 mg/kg in 3 somministrazioni - diltiazem . Iniziando con basse dosi ed incrementando fina alla massima dose tollerata Effetti collaterali: ipotensione sistemica; edema periferico; epatotossicità European Heart Journal (2004) 25, 2243–2278 Current Pediatric Therapy
IPP: Terapia vasoattiva Prostacicline ed analoghi • rilassamento muscolare acuto; • inibizione dell’aggregazione piastrinica; • riparazione del danno endoteliale; • Inibizione del rimodellamento vascolare; • facilitazione nella clearance dell’ET-1; • effetto inotropo; • facilitazione dello scambio periferico di O2. European Heart Journal (2004) 25, 2243–2278
IPP: Terapia vasoattiva Prostacicline ed analoghi • I più utilizzati: • epoprostenol: in infusione continua alla dose iniziale di 2 ng/kg/min fino a 20-40 ng/kg/min (50 ng/kg/min); • Treprostinil; • iloprost : aerosol 2,5-5 ng in 10-15 min per 4 vv/die; Effetti avversi: cefalea, flushing, dolori articolari ed agli arti, dolore toracico, nausea, vomito, diarrea, ipotensione European Heart Journal (2004) 25, 2243–2278 Current Pediatric Therapy
Epoprostenol and Home Mechanical Ventilation for Pulmonary Hypertension Associated With Chronic Lung Disease Ali N. Zaidi, MD, Michael D. Dettorre, DO, Gary D. Ceneviva, MD, and Neal J. Thomas, MD, MS Pulmonary hypertension (PH) can be associated with bronchopulmonary dysplasia (BPD) of infancy, and mortality in these pediatric patients is high without aggressive medical treatment. Continuous intravenous epoprostenol (prostacyclin) was shown to lower pulmonary artery pressures (PAP) in children with idiopathic pulmonary arterial hypertension (PAH), formerly referred to as primary pulmonary hypertension. We report on the first case of long-term home ventilation in combination with chronic intravenous epoprostenol in a child with severe pulmonary hypertension associated with chronic lung disease. This aggressive combination resulted in significant improvement in pulmonary artery pressures, substantial improvement in quality of life, and eventual discontinuation of home ventilation. Pediatric Pulmonology 40:265–269 (2005)
Magnesium sulfate for persistent pulmonary hypertension of the newborn Ho JJ, Rasa G Background: Persistent pulmonary hypertension of the newborn (PPHN) occurs in approximately 1.9 per 1000 newborns and may be more frequent in developing countries. There is strong evidence for the use of inhaled nitric oxide (iNO) and extra corporeal membrane oxygenation (ECMO) in the treatment of PPHN. However, many developing countries do not have access or the technical expertise required for these expensive therapies. Magnesium sulfate is a potent vasodilator and hence has the potential to reduce the high pulmonary arterial pressures associated with PPHN. If magnesium sulfate were found to be effective in the treatment of PPHN, this could be a cost effective and potentially life-saving therapy. Objectives: To evaluate the use ofmagnesiumsulfate compared with placebo or standard ventilatormanagement alone, sildenafil infusion, adenosine infusion, or inhaled nitric oxide on mortality or the use of backup iNO or ECMO in term and near-term newborns (> 34 weeks gestational age) with PPHN. Search strategy: The standard search strategy of the Cochrane Neonatal Review Group (CNRG) was used. No language restrictions was applied. The Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 1, 2006) and MEDLINE (1966 to April 20, 2007) were searched for relevant randomized and quasi-randomized trials. In addition the reference lists ofretrieved articles were reviewed and known experts were contacted to obtain unpublished data. The Cochrane Database Systematic reviews 2007, Issue 3
Types of studies: Randomized or quasi-randomized studies. Types of participants: Term and near term neonates (> 34 weeks gestation at birth and < 1 month of age) with PPHN diagnosed by degree of hypoxia [such as PaO2 of less than 50 mmHg or 6.67 kPa or Oxygenation Index (OI) > 25] or echocardiographic criteria. Types of intervention: Magnesium sulfate infusion of any dose or duration. The comparison group would be: Placebo or standard ventilator management alone; Sildenafil infusion; Adenosine infusion; Inhaled nitric oxide Both groups may or may not be on assisted ventilation. Treatment backup with iNO and ECMO was allowed in either group. Primary outcomes: 1. All cause mortality to hospital discharge or 28 days of age 2. Use of inhaled nitric oxide or ECMO 3. Mortality or the use of backup therapy (iNO or ECMO) Secondary outcomes: 1. Failure to improve oxygenation within 30 to 60 minutes (dichotomous variable) 2. Short term effect on oxygenation index and arterial PO2 after therapy (both absolute values and change from baseline). 3. Neurodisability (> 2 standard deviation below the mean on a validated assessment tool) in first year of life 4. Neurodisability (> 2 standard deviation below the mean on a validated assessment tool) in childhood and beyond 5. Cerebral palsy on physician assessment 6. Hearing impairment 7. Duration of hospital stay (days) 8. Adverse effects such as hypocalcaemia and hypokalemia, cardiac arrhythmias and severe hypotension Main results: No eligible trials were found Authors’ conclusions: On the basis of the current lack of evidence, the use of magnesium sulphate cannot be recommended in the treatment of PPHN.Randomised controlled trials are recommended. The Cochrane Database Systematic reviews 2007, Issue 3
Ritornando alla nostra bambina
Terapia Fentanil, Midazolam a cui è stato aggiunto Cisatracurium Ventilazione: SIPPV poi HFOV FiO2 50; MAP 26 cmH2O; frequenza di 7 Hz Soldesam Ampicillina/sulbactam e Meropenem Plasma, Igvena Furosemide; Dopamina NO (20 ppm) 27/1 PAPs 60-65 mmHg
Sildenafil:0,3 mg/kg/dose x 3 vv/die 29/1 PAPs 85 mmHg 31/1 al 4 /2: PAPs 60 mmHg Aminofillina 5 mg ev NO in scalo 4/2:Broncoaspirato: Stenotrophomonas maltophilia 5/2: Teicoplanina e Amikacina 7/02: PAPs 95-100 mmHg 7/2: Emocromo: 3270000, Hb 92,, GB 21,6000 (N69%, E1%, L24%, M6%) PTL 108.000. PCR:8,78 Broncoaspirato: Pseudomonas Glazidim 10/2: emocultura: Stenotrophomonas Maltophilia 10/2 PAPs 95-100 mmHg 18-21/2 PAPs 55-60 mmHg 11/2 Bosentan 15 mgx 2
15/2 Si modifica mosalità ventilatoria con SIMV con i seguenti parametri: PIP 25; PEEP 4; frequenza sett 35 atti/min; FiO2 40% 19/2 sospeso NO 3/3: la piccola viene estubata ed avviata ventilazione NCPAP con PEEP 4 cmH2O, FiO225% In atto è in respiro spontaneo, in culletta a cielo aperto con O2 a 0.5 L/min 8/3: PAPs 45-50 mmHg 9/3: avviato svezzamento dal bosentan