Download
1 / 20
200 likes | 321 Views
Cardiovascular Risk Factors. Non-modifiable Age Gender Family History. Modifiable Hypertension Smoking Diabetes Hyperlipedemia Other: Homocystine levels CRP levels Sedentary life style obesity. Cardiovascular Evaluation. History Blood Pressure Pulse Auscultation CXR EKG

E N D
Cardiovascular Risk Factors • Non-modifiable • Age • Gender • Family History • Modifiable • Hypertension • Smoking • Diabetes • Hyperlipedemia • Other: • Homocystine levels • CRP levels • Sedentary life style • obesity
Cardiovascular Evaluation • History • Blood Pressure • Pulse • Auscultation • CXR • EKG • Stress EKG • Scintigraphy – Thallium • Echocardiograms • Angiography
Exercise Stress Testing • Pathophysiology: • At rest, there may be adequate coronary blood flow, with exercise, supply may not keep up with demand leading to characteristic ST segment changes and other end points due to obstruction. • At least a 70-80%occlucions is needed before coronary stenosis (obstruction) is reliably detected by this test. • Significant coronary artery disease can exist with a negative Exercise Stress Test.
Indications for Stress Testing • Evaluation of patients with suspected coronary artery disease (CAD). • Typical Angina Pectoris • Atypical Angina Pectoris • Evaluation of patients with known coronary artery disease (CAD). • After myocardial infarction • After intervention • Evaluation of exercise capacity • Evaluation of cardiac rhythm disorders
Preparation for Stress Testing • History • Type, character, durations, radiation, position of chest pain • Factors that increase or decrease chest pain • Associated symptoms i.e. SOB, Diaphoresis, leg pain, etc • Other illnesses: - HTN, DM, COPD, >lipids, CNS disease, Physical Limitations • Medications • General Activity level
Preparation for Stress Testing • Physical Examination • General appearance, gait and mobility • Cardiac auscultation and palpation • Pulmonary Exam • Vascular- bruits, pulses • Musculoskeletal – limb strength and mobility • Laboratory Studies • Screening chemistry and hematologic profiles • Resting ECG
Contraindications to Stress Testing • Acute myocardial infarction or unstable angina • Acute cardiac inflammation, pericarditis, endocarditis, or myocarditis • Severe congestive heart failure • Uncontrolled sustained ventricular arrhythmias, symptomatic supraventricular arrhythmias or high-grade block • Hemodynamically significant aortic stenosis
Contraindications to Stress Testing • Severe hypertension (>200/>100) • Active thromboembolic processes within past 3 months • Pulmonary embolism • Deep vein thrombosis • Poor candidate for exercise • Extreme obesity, i.e. Exceeds equipment capacity, usually can’t do over 350 lb. • Severe mental or physical disabilities
Possible Contraindications to Stress Testing based on Resting ECG • ST-segment changes 1 mm or greater, either depression or elevation • Ventricular strain patterns or hypertrophy • T-wave inversions • Left bundle branch block • Right bundle branch block, if significant • Prolonged QT interval
Equipment for Stress Testing • Treadmill or bicycle or steps • ECG machine • Blood Pressure Cuff • Computer is a ‘nice to have’ • ACLS Certification • Exit Strategy • Good Help* (it takes two to test)
Normal Response to Stress Testing • Heart rate increases • Blood pressure increases • Cardiac output increases • Total peripheral resistance decreases • Dysrhythmias – isolated unifocal PVC’s and PAC’s not of concern, usually suppressed at increased heart rate • Oxygen consumption increases (1MET = 3.5 ml O2/Kg./min = 1 metabolic equivalent)
Abnormal Response to Stress Testing • Heart rate fails to rise above 120 or unable to attain target heart rate of 85% of max • Blood pressure shows a drop in systolic • Patient physically unable to complete test • Marked hypertension, >260/115 • Chest Pain and/or unusual shortness of breath
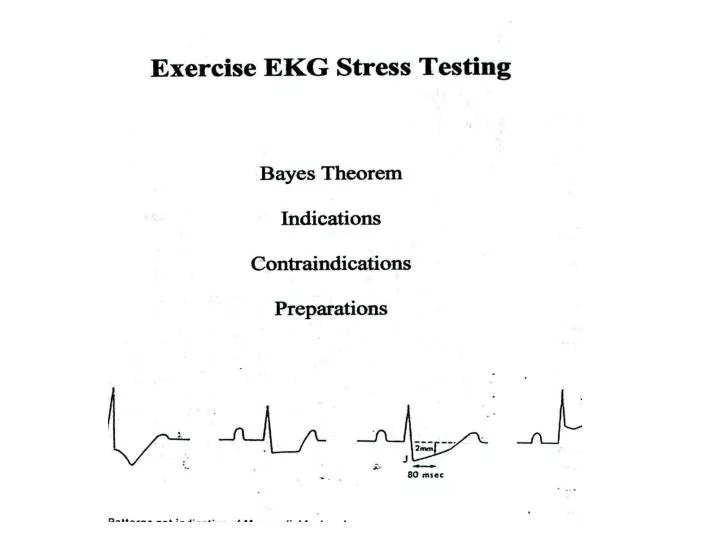
Normal Response of ECG to Stress Testing • ECG Changes • QRS complex decreases in size • J point depresses, resulting in up sloping of ST segment • ST segment returns to baseline by 80 milliseconds • PR segment may down slope – thus baseline is defined as PQ junction • R amplitude may decreaseat rates that go above 130 • T wave decreases
Abnormal Response of ECG to Stress Testing • ECG Changes • Horizontal or down sloping ST segments • ST segment depressed or elevated • ST segment does not return to baseline by 80 milliseconds • U or T wave inversion • Dysrhythmias – rate dependent blocks above first degree, WPW appears, Atrial fib/flutter, multiform and/or increasing PVC’s, V-tach occurs
Protocols • EST’s utilize standard protocols to progressively increase cardiovascular work load in a uniform and reproducible manner. • Work load is expressed in METS (1 MET = 3.5ml O2 /Kg/min). • 1 MET (3.5 ml) = basal O2 requirement • 5 METS (17.5 ml) = activities of daily life • 13 METS (45.5 ml) = good work out and excellent prognosis • Myocardial O2 consumption is estimated by multiplying HR by BP to obtain the ‘double product’. • Double product < 20,000 is low heart work load • Double product > 29,000 indicates high heart work load
Reasons to Terminate Test • Absolute • Patient requests to stop • Technical/mechanical difficulties • Suspected MI • CNS symptoms • Serious dysrhythmias • Drop in systolic BP • Severe Angina • ST elevation > 1mm • Poor perfusion • Relative • > 2mm of ST depression • Increasing chest pain • Tired or SOB • Wheezing • Claudication • SVT • SBP>260, DBP>115 • Exercise induced BBB • 85% of max predicted HR • > 15 METS • > 30,000 double product