Download
1 / 9
90 likes | 171 Views
Binational Health Insurance Models APHA 2008 Annual Meeting William H. Dow Henry J. Kaiser Associate Professor of Health Economics UC-Berkeley. Binational Health Insurance Background. What is it? Insurance that provides benefits across 2 countries (U.S., Mexico) Why important?

E N D
Binational Health Insurance ModelsAPHA 2008 Annual MeetingWilliam H. DowHenry J. Kaiser Associate Professor of Health EconomicsUC-Berkeley
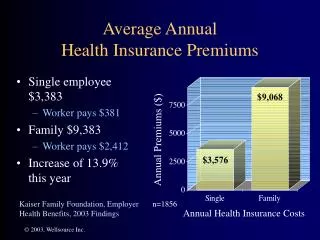
Binational Health Insurance Background • What is it? • Insurance that provides benefits across 2 countries (U.S., Mexico) • Why important? • Uninsurance leads to catastrophic expenditures, stress, worse health • Of ~11 million Mexican-born in the U.S., ~6 million are uninsured. => Need new initiatives.
Potential Benefits of BINATIONAL Health Insurance • Binational service delivery: • Cost savings from contracting providers in Mexico. [30-50%?] • Health benefits of better, culturally competent care, and potentially integrated care for migrants. [Unlikely?] • Labor market efficiency, by facilitating worker and family mobility. • Binational financing: • Health system efficiency: Take currently fragmented financing for separate care delivery systems, and redirect toward an integrated insurance product with more preventive care, etc. • Health financing equity: More explicitly planned approach to sharing financing burdens.
Binational Health Insurance Challenges • Financing: • Most uninsured will need premium subsidies. • New funds needed from outside system. • Low demand for insurance: • Need large subsidies, well marketed, easy to understand, and non-threatening for undocumented. • Geography: lower expected benefit if do not live near border. • Adverse selection expected. Role of mandates? • Regulatory barriers: • Insurance, credentialing. • Administrative barriers: • Few promising models for well-integrated care across systems…so unlikely to be realized soon. • Political barriers: • Resistance to financing care of immigrants or emigrants. Migrants fall through cracks without international agreements.
BHI Potential Varies by Group • Groups with current BHI take-up: • Non-poor documenteds living in border areas (lower premiums, scale economies). • Circular migrants with large employers (farmworkers). • Groups with low potential take-up: • Low-income: Unless highly subsidized. • Undocumenteds (unless subsidized or employer mandated). • Living far from border (if seriously ill, they can return to Mexico and enroll in Seguro Popular at that time)
Building Blocks for BHI:United States • Insurance: • Employer-sponsored insurance: • Premium tax subsidies of 15%-35%. • Large firms: administrative savings, high take-up, low adverse selection. • But insurance paid with lower wages. • Individual insurance: • inefficient, with selection problems. Bad model for BHI? • Medicaid/SCHIP: • low-income pregnant women, documented children. • Kaiser: • $8 PMPM for undocumented kids < 250% FPL in California. • Fragmented safety net for uninsured: • Hospitals, clinics funded by: federal DSH and FQHC, state, counties, non-profits, pharma drug discounts.
Building Blocks for BHI:Mexico • IMSS: social security insurance for formal sector workers. • Seguro Popular: new government insurance for non-IMSS, highly subsidized. • SSA Ministry of Health: safety net clinics, hospitals.
Some Options for Financing Subsidized BHI • Redirect existing subsidies for uninsured: • DSH, FQHC, state, county, Mexican SSA, private pharma, etc. • Negotiate explicit financing responsibilities. E.g., U.S. govt pays larger share, the longer migrant is in U.S.? • Reduce costs via: • Strong incentives for using lower cost providers • “Medical tourism” contracts for expensive care. • Medical home to coordinate chronic care. • Role of mandates in migration reform? • Individual mandate for immigrant health insurance (with sufficient subsidies): can reduce adverse selection, raise political will. • Employer mandate can reduce costs (at risk of labor market distortion): lower admin costs, AND capture tax subsidy.
Piloting Subsidized BHI • Estimate demand increases, cost offsets. • Need large subsidies for initial pilot (foundation)? • Choose border area: • Economies of scale • Allow to test how border-crossing varies by distance (interacted with cost-sharing, quality) • Detailed study of changing safety net financing.