Download
1 / 1
10 likes | 173 Views
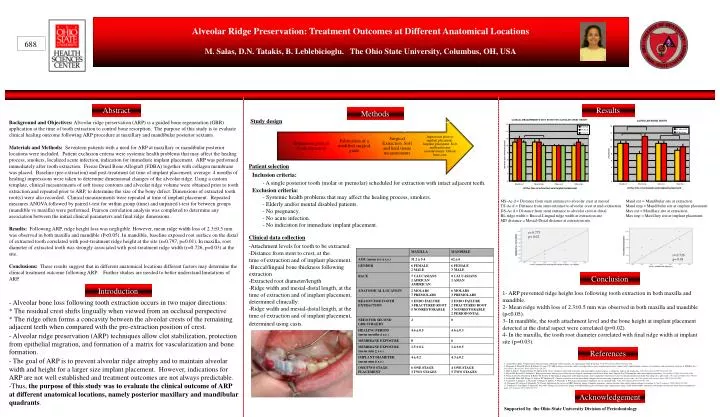
Alveolar Ridge Preservation: Treatment Outcomes at Different Anatomical Locations M. Salas, D.N. Tatakis, B. Leblebicioglu. The Ohio State University, Columbus, OH, USA. 688. Abstract. Results. Methods. Study design.

E N D
Alveolar Ridge Preservation: Treatment Outcomes at Different Anatomical Locations M. Salas, D.N. Tatakis, B. Leblebicioglu. The Ohio State University, Columbus, OH, USA 688 Abstract Results Methods Study design Background and Objectives: Alveolar ridge preservation (ARP) is a guided bone regeneration (GBR) application at the time of tooth extraction to control bone resorption. The purpose of this study is to evaluate clinical healing outcome following ARP procedure at maxillary and mandibular posterior sextants. Materials and Methods: Seventeen patients with a need for ARP at maxillary or mandibular posterior locations were included. Patient exclusion criteria were systemic health problems that may affect the healing process, smokers, localized acute infection, indication for immediate implant placement. ARP was performed immediately after tooth extraction. Freeze Dried Bone Allograft (FDBA) together with collagen membrane was placed. Baseline (pre-extraction) and post-treatment (at time of implant placement; average: 4 months of healing) impressions were taken to determine dimensional changes of the alveolar ridge. Using a custom template, clinical measurements of soft tissue contours and alveolar ridge volume were obtained prior to tooth extraction and repeated prior to ARP, to determine the size of the bony defect. Dimensions of extracted tooth root(s) were also recorded. Clinical measurements were repeated at time of implant placement. Repeated measures ANOVA followed by paired t-test for within group (time) and unpaired t-test for between groups (mandible vs maxilla) were performed. Pearson correlation analysis was completed to determine any association between the initial clinical parameters and final ridge dimensions. Results: Following ARP, ridge height loss was negligible. However, mean ridge width loss of 2.30.5 mm was observed in both maxilla and mandible (P<0.05). In mandible, baseline exposed root surface on the distal of extracted tooth correlated with post-treatment ridge height at the site (r=0.797, p=0.01). In maxilla, root diameter of extracted tooth was strongly associated with post-treatment ridge width (r=0.726, p=0.03) at the site. Conclusions: These results suggest that in different anatomical locations different factors may determine the clinical treatment outcome following ARP. Further studies are needed to better understand limitations of ARP. Patient selection • Inclusion criteria: • A single posterior tooth (molar or premolar) scheduled for extraction with intact adjacent teeth. • Exclusion criteria: • Systemic health problems that may affect the healing process, smokers. • Elderly and/or mental disabled patients. • No pregnancy. • No acute infection. • No indication for immediate implant placement. MS-Ac d = Distance from stent entrance to alveolar crest at mesial Mand ext = Mandibular site at extraction TS-Ac d = Distance from stent entrance to alveolar crest at mid-extraction Mand imp = Mandibular site at implant placement DS-Ac d = Distance from stent entrance to alveolar crest at distal Max ext = Maxillary site at extraction BL ridge width = Buccal-Lingual ridge width at extraction site Max imp = Maxillary site at implant placement MD distance = Mesial-Distal distance at extraction site r= 0.773 p= 0.02 Clinical data collection • Attachment levels for tooth to be extracted. • Distance from stent to crest, at the • time of extraction and of implant placement. • Buccal/lingual bone thickness following • extraction • -Extracted root diameter/length • -Ridge width and mesial-distal length, at the time of extraction and of implant placement, determined clinically. • -Ridge width and mesial-distal length, at the time of extraction and of implant placement, determined using casts. r= 0.726 p= 0.03 Conclusion Introduction 1- ARP prevented ridge height loss following tooth extraction in both maxilla and mandible. 2- Mean ridge width loss of 2.30.5 mm was observed in both maxilla and mandible (p<0.05). 3- In mandible, the tooth attachment level and the bone height at implant placement detected at the distal aspect were correlated (p=0.02). 4- In the maxilla, the tooth root diameter correlated with final ridge width at implant site (p=0.03). • Alveolar bone loss following tooth extraction occurs in two major directions: • * The residual crest shifts lingually when viewed from an occlusal perspective • * The ridge often forms a concavity between the alveolar crests of the remaining adjacent teeth when compared with the pre-extraction position of crest. • - Alveolar ridge preservation (ARP) techniques allow clot stabilization, protection from epithelial migration, and formation of a matrix for vascularization and bone formation. • - The goal of ARP is to prevent alveolar ridge atrophy and to maintain alveolar width and height for a larger size implant placement. However, indications for ARP are not well established and treatment outcomes are not always predictable. • Thus, the purpose of this study was to evaluate the clinical outcome of ARP at different anatomical locations, namely posterior maxillary and mandibular quadrants. References 1. Araujo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol 2005;32(2):212-218. 2. Brugnami F, Then PR, Moroi H, Kabani S, Leone CW. GBR in human extraction sockets and ridge defects prior to implant placement: clinical results and histologic evidence of osteoblastic and osteoclastic activities in DFDBA. Int J Periodontics Restorative Dent 1999;19(3):259-267. 3. Fickl S, Zuhr O, Wachtel H, Bolz W, Huerzeler M. Tissue alterations after tooth extraction with and without surgical trauma: a volumetric study in the beagle dog. J Clin Periodontol 2008;35(4):356-363. 4. Fowler EB, Breault LG, Rebitski G. Ridge preservation utilizing an acellular dermal allograft and demineralized freeze-dried bone allograft: Part II. Immediate endosseous implant placement. J Periodontol 2000;71(8):1360-1364. 5. Froum S, Cho SC, Rosenberg E, Rohrer M, Tarnow D. Histological comparison of healing extraction sockets implanted with bioactive glass or demineralized freeze-dried bone allograft: a pilot study. J Periodontol 2002;73(1):94-102. 8. Lyford RH, Mills MP, Knapp CI, Scheyer ET, Mellonig JT. Clinical evaluation of freeze-dried block allografts for alveolar ridge augmentation: a case series. Int J Periodontics Restorative Dent 2003;23(5):417-425. 9. Yamamoto T, Ishikawa A, Watanabe Y, Hirano N, Shibata Y, Watanabe T. Prevalence of horizontal attachment loss in extracted teeth. J Clin Periodontol 2004;31(9):791-795. 10. Zitzmann NU, Scharer P, Marinello CP. Factors influencing the success of GBR. Smoking, timing of implant placement, implant location, bone quality and provisional restoration. J Clin Periodontol 1999;26(10):673-682. 11. Zubillaga G, Von Hagen S, Simon BI, Deasy MJ. Changes in alveolar bone height and width following post-extraction ridge augmentation using a fixed bioabsorbable membrane and demineralized freeze-dried bone osteoinductive graft. J Periodontol 2003;74(7):965-975. Acknowledgement Supported by the Ohio State University Division of Periodontology