Download
1 / 117
1.24k likes | 1.59k Views
Liver MSc Clinical Biochemistry. Dr Sarah Mapplebeck Consultant Clinical Biochemist. Lecture structure. Session 1 Liver structure and function Liver investigations Session 2 Liver cases. Session 1. STRUCTURE AND FUNCTION. Structure of liver. Largest internal organ

E N D
LiverMSc Clinical Biochemistry Dr Sarah Mapplebeck Consultant Clinical Biochemist
Lecture structure • Session 1 • Liver structure and function • Liver investigations • Session 2 • Liver cases
Session 1 STRUCTURE AND FUNCTION
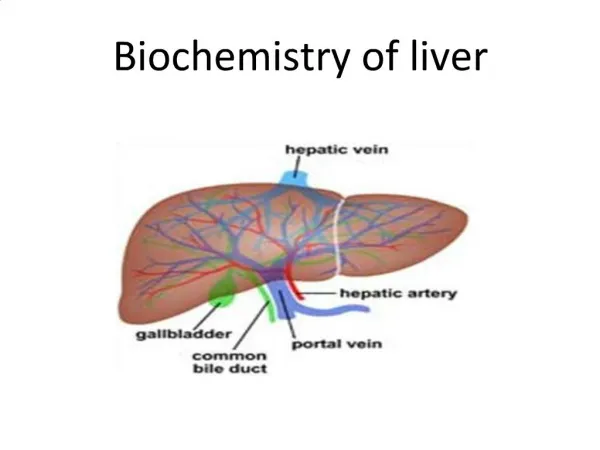
Structure of liver • Largest internal organ • Situated in right hypochnodrium • Divided into right and left lobes by middle hepatic vein • Subdivided into eight segments by divisions of the right, middle and left hepatic vein
Blood supply • Blood supply to liver constitutes 25% of resting cardiac output via two main vessels • Hepatic artery • Branch of coeliac axis • Supplies 25% of total blood flow • Autoregulation of blood flow by hepatic artery ensure a constant total liver blood flow • Portal vein • Drains most of the GI tract and spleen • Supplies 75% of blood flow
Functions of the liver • Metabolic • Protein metabolism • Carbohydrate metabolism • Lipid metabolism • Formation of bile • Metabolism and excretion of bilirubin • Hormone and drug inactivation
Protein metabolism • Synthesis • Principal site of synthesis of most circulating proteins • Receives amino acids from intestine and muscle and regulates plasma levels • Plasma contains approx 60-80 g/L (albumin, globulin, fibrinogen) • Transport proteins e.g transferrin, caeruloplasmin produced in liver • Coagulation factors and complement components • Degradation (nitrogen excretion) • Amino acids degraded by transamination and oxidative deamination to ammonia • Ammonia converted to urea and is renally excreted • Failure of excretion occurs in severe liver disease
Carbohydrate metabolism • Glucose homeostasis and maintenance of blood sugar major function of liver • Stores approx 80g glycogen • Immediate fasting state • Blood glucose maintained by glucose released from glycogen breakdown (glycogenolysis) or by newly synthesized glucose (gluconeogensis) • Sources for gluconeogensis are lactate, pyruvate, amino acids from muscle (alanine and glutamine) • Prolonged starvation • Ketone bodies and fatty acids are used as alternative sources of fuel • Body adapts to lower glucose requirement
Lipid metabolism • Fats transported in plasma as lipoproteins (protein-lipid complexes) • Liver has major role in metabolism of lipoproteins • VLDL and HDL synthesised by liver • Triglycerides (come from diet) also synthesised in liver from circulating free fatty acids and glycerol • Cholesterol comes from diet but mainly synthesised in liver from acetyl CoA
Formation of bile • Bile secretion • Bile acid metabolism • Bilirubin metabolism
Bile secretion • Bile consists of water, electrolytes, bile acids, cholesterol, phospholipids and conjugated bilirubin • Two processed involved in bile acid secretion • Bile salt dependent • Bile salt independent • Bile salt dependent • Uptake of bile acids (and other organic/inorganic ions) across the basolateral (sinusoidal) by transport proteins – driven by Na-K-ATPase in basolateral membrane • Sodium and water follow passage of bile acids • Bile salt independent • Water flow is due to other osmotically active solutes e.g glutathione, bicarbonate
Bile acid metabolism • Bile acids are synthesised in hepatocytes from cholesterol • Excreted into the bile and pass into duodenum • Primary bile acids • Cholic acid and chenodeoxycholic acid are conjugated with glycine or taurine which increases their solubility • Secondary bile acids • Primary bile acids converted by intestinal bacteria into deoxycholic and lithocholic acid • Bile acids act as detergents – main function lipid solubilisation • Have both hydrophobic and hydrophilic end and in aq solution aggregate forming micelles
Hormone and drug inactivation • Major site for metabolism of drugs and alcohol • Fat soluble drugs are converted to water soluble substances facilitating excretion in bile or urine • Liver catabolises hormones e.g insulin, glycogen, oestrogens, growth hormone, glucocorticoids, parathyroid hormone • Prime target organ for hormones e.g insulin
Bilirubin metabolism • Produced mainly from breakdown of mature red cells in Kupffer cells of liver and reticuloendothelial cells • 15% bilirubin comes from catabolism of other haem containing proteins (myoglobin, cytochromes, catalases) • Typically 250-300mg bilirubin produced daily • Iron and globulin removed from the haem and reused • Biliverdin is formed from the haem and is reduced to form bilirubin • Bilirubin produced is unconjugated
Bilirubin metabolism • Uncongugated bilirubin • Not water soluble • Transported to liver bound to albumin • Dissociates from albumin and taken up by hepatic cell membrane and transported to ER • In ER is conjugated with glucuronic acid by bilirubin-uridyl diphosphate (UDP)
Bilirubin metabolism • Conjugated bilirubin • Water soluble • Secreted into biliary canaliculi reaching small intestine • In gut bilirubin converted into urobilinogen (colorless) • Most urobilinogen oxidised in colon to brown pigment stercobilin excreted in stool • Some urobilinogen is absorbed from gut into portal blood and small amount excreted in urine
Investigations • Blood tests • Liver function tests • Serum albumin • Prothrombin time • Liver biochemistry • ALT/AST – reflecting hepatocellular damage • ALP and GGT – reflecting cholestasis • Total protein • Viral markers • Additional blood investigations; haematological, biochemical, immunological and genetic • Urine tests • For bilirubin and urobilinogen • Imaging techniques • To define gross anatomy • Liver biopsy • For histology
Liver function tests • Serum albumin • Marker of synthetic function • Guide to severity of chronic liver disease • Falling serum albumin is poor prognostic sign • In acute liver disease albumin may be normal • Prothrombin time (PTT) • Marker synthetic function • Short half life so sensitive indicator of both acute and chronic liver disease • Vit K def should be excluded as cause of prolonged PTT • Vit K def commonly occurs in biliary obstruction as low intestinal concentration of bile salts results in poor absorption of vit K • INR often used as PTT varies in laboratories
Causes of hypoalbuminaemia • Haemodilution • Pregnancy, iv therapy, cirrhosis, antidiuretics • Decreased synthesis • Severe liver disease (chronic hepatitis, cirrhosis) • Malabsorption, malnutrition • Altered distribution • Liver failure/cirrhosis • Malignancy • Loss from the body • Skin (burns, exudative lesions) • Gut (protein loosing enteropathy) • Increased catabolism • Malignancy • Misc • Acute/chronic illness, malignancy
Hyperalbuminaemia • Increased albumin • Dehydration/haemoconcentration • Venous stasis • Healthy young adult
Liver biochemistry • Bilirubin • Aminotransferases • alanine amino transferase (ALT) and asparate amino transferase (AST) • Alkaline phosphatase (ALP) • Gamma glutamly transpeptidase • Total protein
Bilirubin and jaundice • Yellow discoloration of tissues due to bilirubin deposition • Clinical jaundice may not be clear until plasma bilirubin >50 umol/L • First observed in sclera of the eye
Laboratory investigation of Jaundice • Classified on basis of other LFTs • Isolated hyperbilirubinaemia • High serum bilirubin only abnormality • Unconjugated • Conjugated • Hepatobiliary disease • High bilirubin accompanies other abnormalities in LFTs
Isolated hyperbilirubinaemia • Increased production • Haemolytic anaemias, hypersplenism, mechanical heart valves, resorption of haematomas, • Decreased hepatic uptake • Gilbert’s syndrome • Drugs- Rifampicin, Testosterone, Sulphasalazine • Decreased conjugation • Gilbert’s syndrome • Gallstones
Further investigation • Bilirubin fractionation • Conjugated, unconjugated or mixed hyperbilirubinaemia • FBC • Haemolytic disease and pernicious anaemia (megaloblastic anaemia) • Associated with mild isolated hyperbilirubinaemia • Reticulocytes • Haemolytic disease does not always produce low Hb • High retic indicated high red cell production rate seen in haemolytic disease • Lactate dehydrogenase • Elevated in haemolysis, pernicious anaemia and hepatitis • Haptoglobulin • Bind to haemoglobin released in intravascular haemolysis causing low levels
Gilberts syndrome • Autosomal dominant (7% population) • Bilirubin between 20 and 60 μmol/L • Decreased conjugation especially during intercurrent illness or starvation • Elevation <100 umol/L • Measure Conjugated and unconjugated bilirubin • Reflexed in lab on all GP requests when total bilirubin is over 30 umol/L and no other abnormalities • >75 % unconjugated is consistent with Gilberts Syndrome • Become jaundiced when unwell or fasting • Reassure that no further tests are required
Cholestatic jaundice • Extrahepatic cholestasis • Due to large duct obstruction of bile flow at any point in the biliary tract distal to the bile canaliculi • Intrahepatic cholestasis • Failure of bile secretion • Pale stools and dark urine with conjugated serum bilirubin
Transaminases • ALT and AST are present in hepatocytes and leak into blood with liver cell damage • Indicate hepatocellular damage • AST • Mainly mitochondrial and also present in heart, muscle, kidney and brain • High levels seen in hepatic necrosis, MI, muscle injury and CCF • ALT • Cytosol enzyme • More liver specific rise only in liver disease • Released early in liver damage and remain elevated for weeks • In hepatocelluar disease ALT rises before jaundice • Cholestatic disease ALT may not rise • Many labs only measure ALT as more specific than AST
Levels of ALT • Minor elevations (<100 U/L) • Chronic hepatitis B and C • Haemochromatosis • Fatty liver • Moderate elevations (100-300 U/L) • Alcoholic hepatitis • Autoimmune hepatitis • Wilson’s disease • Major elevations (>300 U/L) • Drug toxins e.g. paracetamol • Acute viral hepatitis • Ischaemic liver
Non-hepatic causes of elevated ALT • Coeliac disease • Muscle disease • Strenuous exercise
Alkaline phosphatase (ALP) • Present in canalicular and sinusoidal membranes of liver • Present in other tissues • Bone, intestinal, placenta • Normal situations bone and liver are the major isoenzymes • If required, origin determined by electrophoretic separation of isoenzymes • If elevated GGT, ALP can be presumed to come from liver
Alkaline phosphatase (ALP) • Raised in cholestasis from any cause (intra or extra hepatic) • Synthesis of ALP is increased and realsed into blood • Cholestatic jaundice levels may be 4XURL • Raised levels also in conditions with infiltration of liver e.g metastases and cirrhosis often in absence of jaundice • Highest levels due to liver disease seen with hepatic metastases and primary bilary cirrhosis
Isolated mild rise in Alkaline Phosphatase • Bone disease • Paget’s disease • Osteomalacia • Healing fractures • Metastases • Hyperparathyroidism • Vitamin D deficiency • Drugs • Anti epileptics • Pregnancy • Growth • Children and teenage growth spurt • Biliary disease • Primary biliary cirrhosis (AMA positive)
Other investigations with elevated ALP • Further investigation may include • Calcium and phosphate • VitD and PTH • Liver enzymes • PSA • Electrophoresis • Isoenzymes • Radiology
GGT • Microsomal enzyme present in many tissues as well as liver • Activity can be induced by drugs e.g phenytoin and alcohol • If ALP normal a raised GGT good guide to alcohol intake • Mild elevations in GGT is common even with small alcohol consumption and doesn’t mean liver damage if other liver biochemistry normal • In cholestasis GGT rises in parallel with ALP
Isolated rise in Gamma GT • Only measure to clarify raised alkaline phosphatase or DVLA fitness to drive • Alcohol (although not always) • Drugs • Anticonvulsants, NSAIDs, antibiotics, antifungals, cytotoxics, testosterone • Non alcoholic fatty liver • Congestive cardiac failure • Afro-Caribbeans have higher reference range • Main use to identify source of ALP cheaper the ALP isoenzymes
Other liver function tests • Total proteins • Measurement alone is of little value • Globulin fraction calculated • Elevated globulin fraction is liver disease is usually polyclonal due to increased circulating immunoglobins (rather than monoclonal in myeloma) • Viral markers • Viruses are major cause of liver diease • Virology investigations are often key in diagnosis e.g. hepatitis
Additional blood investigations - Biochemical • Alpha1 antitrypsin • Deficiency can produce cirrhosis • Alpha fetoprotein • Normally produced by fetal liver • Reappearance in high conc indicates hepatocellular carcinoma • Serum and urine copper • Wilsons disease
Additional blood investigations - Immunoglobulins • Increased serum immunoglobulins • Due to reduced phagocytosis by sinusoidal and Kupffer cells of antigen from the gut • Antigens then stimulate antibody production • Immunoglobulins (not produced by liver) • Polyclonal elevations in chronic liver disease • IgM elevated in primary biliary cirrhosis (PBC) • IgA elevated in alcoholic liver disease • IgG increased in autoimmune liver disease
Additional blood investigations - Autoantibodies • Anti mitochondrial Antibodies (AMA) • Found in serum in >95% patients primary biliary cirrhosis • Nucleic, smooth muscle, liver/kidney microsomal antibodies • High titre in autoimmune hepatitis • Also in other autoimmune conditions e.g. SLE and liver disease
Other tests • Genetic analysis • HFE in haemochromatosis • Copper transporting ATPast in Wilsons disease • Urine tests • Bilirubin not found in urine in health • Bilirubinuria is due to presence of conjugated (soluble) bilirubin • Found in jaundiced patient with hepatobilary disease • Absence implies that jaundice is due to increased unconjuated bilirubin • Urobilinogen • Little value but suggests haemolysis or hepatic dysfunction of any cause
Imaging techniques • Ultrasound (USS) • Computed tomography (CT) • Magnetic resonance imaging (MRI) • Plain X ray of abdomen • Endoscopy
Liver biopsy • Histological examination of liver used in the differential diagnosis of diffuse or localised parenchymal disease • Can be done day case • Mortality rate <0.02% in good hands • Guided by US or CT when specific lesions need to be biopsied • Minor complications • Usually in first 2hrs • Abdominal or shoulder pain • Minor bleeding • Major complications • Major bleeding • Sepsis