Download
1 / 20
200 likes | 353 Views
Aetiology and Epidemiology of MS. What is multiple sclerosis?.

E N D
What is multiple sclerosis? It is characterised by repeated episodes of inflammation within the central nervous system, resulting in the destruction of the myelin sheath. Alongside the inflammatory process there is axonal loss, cerebral atrophy and formation of black holes.
What is MS? • MS is a disabling neurological disease • MS is an auto-immune disease characterised by episodes of inflammation within the brain and spinal cord (CNS) • Multiple areas of inflammation then become hardened (sclerosis), leading to plaque formation
General observations • Rarely diagnosed under 10 • Most commonly presents between 20 and 40 • More common in women than men • Incidence higher at latitudes further from the equator • Not directly hereditary, but familial link • Not a contagious illness, but viral trigger Compston A. Coles A. Lancet 2002; 359, 9313: 1221-1231
Aetiology • Exact cause(s) unknown • Regarded multifactorial in nature • Environmental factors • Geographical factors • Genetic factors • Viral trigger • Chance • Initial trigger ? • Viral infection in genetically and/or environmentally susceptible individual • Whatever the trigger, damage is caused by a self-perpetuating auto-immune process
Climate : Geology : Nutritional : Infection : Environmental factors • Low temperature • High winter humidity • Solar/cosmic radiation • Radiation/soil type • Heavy metals • Animals fats/fish oils • Cereals • Viral
Geographical factors • More common with increasing distance from the equator • More common in N than S Europe • More common in S than N Australia • In UK, most common in Scottish regions • Very rare in tropics • Migrants to higher or lower risk areas only change risk status if move before age 15 Compston A. 1998. In McAlpine’s Multiple Sclerosis 3rd Edition.
Migration - UK to South Africa Age at Migration 0 – 14 years 15 – 19 years MS Prevalence 12.8 / 105 62.2 / 105 Kurtzke et al. 1970 South African Medical Journal. 44:663-669
Susceptible races: Northern Europeans North Americans White Europeans at highest risk Less susceptible races: Oriental African-Caribbean Asian Hungarian Gypsies Black African and Japanese at lowest risk Racial influence on MS Compston A. 1998. In McAlpine’s Multiple Sclerosis 3rd Edition.
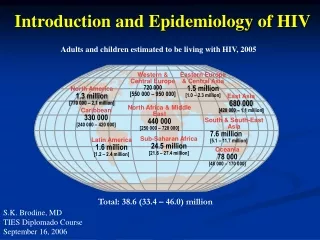
Global epidemiology • Estimates of 2.5 million cases worldwide • Prevalence varies geographically from < 5 per 100,000 to > 150 per 100,000 • prevalence with distance from equator • Highest incidence in temperate climates Compston A. Coles A. Lancet 2002; 359, 9313: 1221-1231 Compston A. 1998. In McAlpine’s Multiple Sclerosis 3rd Edition.
UK epidemiology • Most common cause of neurological disability in young adults in the UK • Affects about 100,000 people in UK • Prevalence between 100-140 per 100,000 in England • Incidence • Around 50 new cases per week in the UK • 2 to 12 per 100,000 population • Not only is the incidence of MS rising, but the incidence of female MS is too. f v m = 3.2 v 1 Compston A. Coles A. Lancet 2002;(359) 9313: 1221-1231 Orton et al 2007);
Suggested UK MS prevalence 1:700 1:1000 1: 1300 1:1300 1:1500
Genetic factors in MS • Gender susceptibility • Genetic component • Not conventionally hereditary • Genetic predisposition • More than one gene responsible (polygenic) • 2 to 1 times more common in women Compston A. Coles A. Lancet 2002;(359) 9313: 1221-1231
Familial risk MS is not directly hereditary, but it can occur in more than one family member • First-degree relations at 20 to 40x risk than general population • 20% of people with MS have a family history • MS risk parent to child 4% • MS risk sibling 4 - 5% • Monozygotic twins at least 300x risk if one twin has MS • The likelihood of the second twin developing it is 30% (Schapiro, 2003) Sadovnick AD. Ebers GC. 1994 International MS Journal:1.1.17-24
Herpes simplex Measles Parainfluenza virus Chlamydia ‘Multiple Sclerosis agent’ Pneumonia Simian Cytomegalovirus Corona virus Epstein-Barr virus HTLV I Simian virus 5 HHV- 6 Viral agents implicated in MS
Epstein Barr Virus • EBV seems to act in adolescence or early adult hood to alter MS susceptibility • The relationship between EBV and MS is firmly established. • 99.5% of people with MS are seropositive for EBV antibodies • Adults who are seronegative for EBV have virtually no risk of developing MS Handel, A.E; Giovannoni, G; Ebers,G.E & Ramagopalan, S.V (2010).
The burden of MS • Natural history studies indicate that it takes a median time of 8, 20 and 30 years to reach the irreversible disability levels of EDSS 4, 6 and 7, respectively (1) • Up to 75% increased annualized divorce rate (2) • Life expectancy is reduced by 5-10 years (3) • In a 2004 study, 2 out of 3 patients with RRMS were unemployed due to the disease (4) 1.Confavreaux, Compston. 2005.[TK] 2. Coles et al. 2001.[TK] 3.Confavreaux, Vukusic. 2006.[TK] 4.Morales-Gonzales. Mult Scler. 2004;10:47-54.
Morbidity in MS • Only about 25 to 30% of people diagnosed with MS will ever need a wheelchair • Takes at least 10 years for patients with RR/SPMS to become wheelchair users • progression is usually more rapid in PPMS Weinshenker et al. Brain 1989; 112:1419-28