Download
1 / 63
640 likes | 656 Views
Physiological mechanisms of regulation of the immune system. Regulation by antigen. Induce immune responses and extinction Affinity maturation of B lymphocytes Maintaining immunological memory Antigenic competition Threshold density of the complex MHC II-gp Ag on APC.

E N D
Regulation by antigen • Induce immune responses and extinction • Affinity maturation of B lymphocytes • Maintaining immunological memory • Antigenic competition • Threshold density of the complex MHC II-gp Ag on APC
Regulation by antibodies • Antibodiescompeteswiththe BCR for antigen (negative regulatorof B lymphocytestimulating) • IgGimmunecomplexesbind to the BCR andFcgR on B cells, resulting in blockingactivationof B lymphocytes • Regulation via idiotypic network
Regulation by cytokines and cellular contact • InteractionAPC - T lymphocyte • InteractionTH1 – macrophages • InteractionTH2 - B lymphocytes • MutualregulationofactivityTH1 versus TH2 • Developmentof leukocyte subpopulations
Regulation by cytokines and cellular contactInteraction between APC and T cell T cell:TCR - antigen-specific receptor CD4 or CD8 - coreceptor (MHCgp binding) CD 28 - costimulatory receptor (binds CD 80, CD 86) CTLA-4 - inhibitory receptor (binds CD 80, CD 86)
Regulation by cytokines and cellular contactInteraction between TH1 and TH2 cells
Negative regulation of effector cells • CTLA-4 - T cell inhibitory receptor, binds ligands CD80 and CD86 • Self-destruction interaction of the apoptotic receptor Fas with ligand FasL on the surface of activated T lymphocytes • Inhibitory receptors of NK cells
Suppression mediated by T lymphocytes • Mutual negative interactionTH1 and TH2cytokine-mediated • Clonaleliminationoranergyof T lymphocytesaftercontactwith antigen on thesurfaceofothercellsthan APC • Regulatory T cells(Treg, Tr1, Th3 - CD 4+) help to maintain tolerance to autoantigens; produceTGFb, IL-10
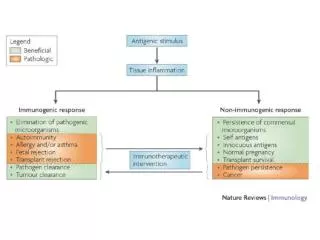
Factors influencing the outcome of the immune response Thesame antigen caninduceanactiveimmune response oranactivestateof tolerance, theresultof response depends on many factors: • Stateoftheimmunesystem • Propertiesof antigen • Doseof antigen • Routeof antigen administration
Cytokines • Regulatory proteins and glycoproteins produced by leukocytes and other cells • Essential regulators of the immune system • Apply also outside the immune system (angiogenesis, tissue regeneration, carcinogenesis, treatment of many brain functions, embryonic development ...) • Cytokines - secreted - membrane (CD 80, CD86, CD40L, FasL ..)
Cytokines • Pleiotropic effect • Operates in a cascade • Cytokine network • Cytokine system is redundant • Effects of cytokines - autocrine - paracrine - endocrine • Are known as interleukins (IL-1…IL-38)(except: TNF, lymphotoxin, TGF, interferons, CSF and growth factors)
B cells communicate via cytokines with other cells, such as T cells and macrophages
Overview of the most important cytokines MF – macrophages; M – monocytes; N – neutrophils; DC – dendritic cells; NK – natural killers; L – lymphocytes; B – B cell; T – T cell
Clasification of cytokines by functions • Proinflammatory cytokines (IL-1, IL-6,IL- 8,IL- 12,IL- 18, TNF) • Antiinflammatory cytokines (IL-4, IL-10, TGF) • Cytokines with the activity of hematopoietic cells growth factor (IL-2, 3, 4, 5, 6, 7, 9, 11, 14, 15, CSF, SCF, LIF, EPO) • Cytokines applying in TH2 humoral immunity (IL-4, 5, 9, 13) • Cytokines applying in the cell-mediated immunity TH1 (IL-2, 12, IFN, GM-CSF, lymphotoxin) • Cytokines with anti-viral effect (IFN-, IFN-, IFN- )
Cytokine receptors • Consistingof 2 or 3 subunits • Onesubunitbindscytokine, other are associatedwithcytoplasmicsignalingmolecules (protein kinases) • Signalingsubunitisshared by severaldifferentcytokinereceptors - called receptor family • Signalingthrough these receptorsmaylead to proliferation, differentiation, activationofeffectormechanismsorblockingthe cell cycleandinductionofapoptosis
Causal treatment a) Stem cell transplantation • treatmentof severe congenitaldisordersoftheimmunesystemandsomelymphoproliferativeandmyeloproliferativedisorders • complications: infectiouscomplicationsGraft-versus-host disease • obtaining stem cells - from bone marrow - fromumbilicalcordblood - fromperipheralblood
Causal treatment b) Gene therapy • transductionof the missing gene to hematopoietic stem cells using viralvectors • used as a treatmentfor 2 formsof SCID
Substitution treatment • autologous stem cell transplantation (following chemotherapy and radiotherapy) • treatment with intravenous immunoglobulin (derived from plasma of blood donors) • substitution of C1 inhibitor for hereditary angioedema • substitution of erythropoietin in patients with chronic renal failure • substitution of G-CSF in agranulocytosis
Immunomodulation = medicalprocedure to adjustthedisruptedimmunefunction Non-specificimmunosuppression • nonspecific = affects not onlyautoreactiveandaloreactivelymphocytes, butalsoothercomponentsofimmunity (risk ofreductionantiinfectiousandantitumorimmunity) • usedfortreatmentofautoimmunediseases, for organ transplantationand severe allergicconditions
Non-specific immunosuppression Corticosteroids • anti-inflammatory, immunosuppressive effects • suppress the expression of some genes (IL-2, IL-1, phospholipase A, MHC gp II, adhesion molecules) • inhibition of histamine release from basophils • higher concentrations induce apoptosis of lymfocytes
Non-specific immunosuppression Immunosuppressants affecting the metabolism of DNA (cytostatics) • cyclophosphamide (alkylating agent) • methotrexate (antimetabolite) • azathioprine (purine analogue)
Non-specificimmunosuppression Immunosuppressantselectivelyinhibiting T cells • immunosuppressive ATB: cyclosporine A, tacrolimus, rapamycin(suppressingtheexpressionof IL-2 and IL-2R in activated T lymphocytes) • anti-CD3 monoclonalantibody(imunosuppressionaftertransplantation, treatmentofrejectioncrises)
Non-specificimmunosuppression Immunoglobulins in the immunosuppressive indication • polyspecific intravenous immunoglobulins • inhibition of B lymphocytes • antiidiotype activity • inhibition of cytokines • neutralization of toxins • inhibition of complement activation
Anti-inflammatory and antiallergic treatment • nonsteroidal anti-inflammatory drugs • antihistamines- blocking H1 receptor - reduce the expression of adhesion molekules - reduce the secretion of histamine ... • inhibitors of inflammatory cytokine- monoclonal antibodies against TNF - thalidomide (TNF inhibitor) • Anti IgE antibodies (omalizumab) - severe allergic astma
Non-specific immunostimulant therapy • synthetic immunomodulators • Methisoprinol (Isoprinosine) - used in viral infections with more severe or relapsing course • bacterial extracts and lysates • Broncho-Vaxom - prevention of recurrent respiratory tract infections • Ribomunyl • products of the immune system • IL-2 - renal adenocarcinoma • IFNa, IFNb - viral hepatitis, some leukemia • Erythropoietin – renal failure • G-CSF, GM-CSF – neutropenia • Transfer factor (blood donors leukocytes undergoing dialysis) • Thymus hormones
Antigen-specific immunomodulation • specificimmunomodulation = induceofanimmune response or tolerance to a specific antigen • activeimmunization • passiveimmunization • specificimmunosuppression
Antigen-specific immunomodulation Activeimmunization (vaccination)= the induction of immunity after exposure toan antigen • activatesspecificcellularandhumoralimmunity • createslong-term immunity (memorycells) • protectagainst a pathogenbearingthis antigen orsimilar antigen (prophylaxis)
Antigen-specific immunomodulation active immunization (vaccination) • vaccines are made from inactivated or attenuated microorganisms or their antigens (polysaccharide capsule, toxins) • attenuated vaccines cannot be used by immunocompromised individuals • risk of infection or anaphylactic reactions
Antigen-specific immunomodulation Passiveimmunization • natural- transfer ofmaternalantibodies in fetalblood • therapeutically - the use ofanimalantibodiesagainstvarioustoxins(snaketoxins, tetanus toxin, botulinum toxin) • prophylaxis - thehumanimmunoglobulinfromimmunizedindividuals (hepatitis A, rabies, tetanus) - Anti-RhDantibodies – preventimmunizationofmotherwithRhD+ fetus erythrocytes • provides a temporary (3 weeks) specifichumoralimmunity • the risk anaphylacticreactions
Antigen-specific immunomodulation Specific immunosuppression= induction of tolerance to a specific antigen • induction of tolerance by oral administration of antigen (treatment of certain autoimmune diseases) • allergen immunotherapy (pollen, insect poisons) Vaccination against cancer • immunization by dendritic cells
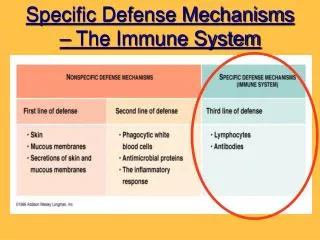
Defence against extracellular pathogens • bacteria (gram-negative, gram-positive cocci, bacilli), unicellularparasites • pathogensinduceinflammation • removed by phagocytosis - neutrophilgranulocytes • opsonization (IgGandIgAantibodies, C3b, lectins, CRP...)
Defence against extracellular pathogensOpsonisation and phagocytosis
Defence against extracellular pathogens • Phagocytes are attracted to thesiteofinfection by chemotacticsubstances(C5a, C3a andchemotacticproductsofbacteria…) • ingestedbacteria are destroyed by themicrobicidalsystems(productsof NADP-H oxidase, hydrolyticenzymesandbactericidalsubstances in lysosomes) • phagocytesproduceproinflammatorycytokines(IL-1, IL-6, TNF)
Defence against extracellular pathogens • IgM - complement activation • IgG - complement activation, opsonization • IgA - opsonizationsIgA prevents against infection by intestinal and respiratory bacteria • in the defense against bacterial toxins apply neutralizing antibodies (Clostridium tetani and botulinum …)
Defence against extracellular pathogens • "indirect toxins - bacterial Lipopolysaccharide (LPS) stimulates big number of monocytes to release TNF, which can cause septic shock • individuals with immunodeficiency of phagocytes, complement and antibodies production are especially at risk of infections with extracellular bacterial
Defense against intracellular pathogens • bacteria, fungi and unicellular parasites • intracellular parasites are resistant to the microbicidal mechanisms of phagocytes • macrophages, which absorbed them, produce IL-12 → TH1 differentiation, production of IFNg and membrane TNF → activation of macrophages and production of NO
Defense against intracellular pathogens • TClymphocytesapply in the defense againstintracelularparasites, whichescapefromphagolysosomes • individualswithcertaindisordersofphagocytesanddefectsof T lymphocytes are at risk ofinfectionswithintracellularmicroorganisms
Anti-viral defence • interferons - productionofIFNaandIFNbisinduced in infectedcells; IFNgactivatesmacrophages (iNOS) • IFNaandIFNb -preventsviralreplication - induceproliferationofNK cells - increase the expression of HLA-I
Anti-viral defence • NK cells - ADCC (Antibody-dependent cell-mediated cytotoxicity); NK cell bind with CD16 (Fcg receptor) to IgG which has bound to the surface of infected cell and then NK cell release perforins and granzymes (degranulation) • infected macrophages produce IL-12 (a strong activator of NK cells)
Anti-viral defence • in the defense againstcytopathicvirusesappliedantibodies: • sIgAinhibitmucosaladhesionofviruses (defense againstrespiratoryvirusesandenteroviruses) • neutralizingIgGandIgMantibodiesactivatetheclassicalpathwayofcomplement, thatisable to lyse certainviruses • opsonizedviralparticles are phagocytosed • IgAandIgGhavepreventiveeffect in secondaryviralinfection