Download
1 / 70
750 likes | 1.18k Views
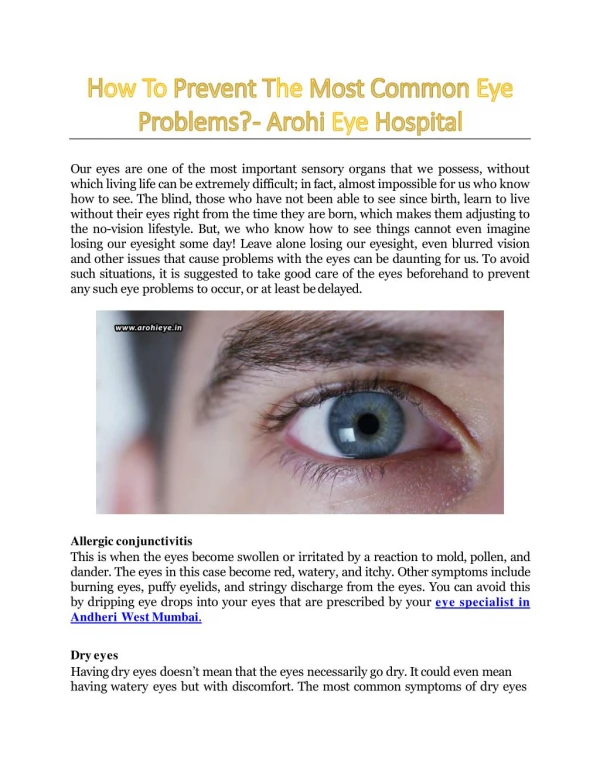
Drugs for Common Eye Problems. Cecilia A. Jimeno, M.D. Ateneo School ond Medicine & Public Health. Anatomy & Physiology. Topical Ophthalmic Drugs: Considerations. They must be absorbed into the anterior chamber

E N D
Drugs for Common Eye Problems Cecilia A. Jimeno, M.D. Ateneo School ond Medicine & Public Health
Topical Ophthalmic Drugs: Considerations • They must be absorbed into the anterior chamber • They may be administered at different frequencies depending on whether they are in ointment or solution form • Ointments: have a longer duration of action (2-4 hrs) than drops • They must be relatively easy to administer for client compliance
INTRODUCTION: Tips on using Ophthalmological Preparations • Ophthalmological preparations are sterile but once opened they have the potential to be contaminated • Hence, dropper tips should NOT touch any surface • Maximum volume accommodated by the lids is 30μl; usual drop size of a standard eye drop bottle is 20 μl which will stimulate tearing for 5 minutes
TIPS • Only one drop should be placed in the eye at a time since by sheer volume it will just spill over • Allow a 5 minute interval between 2 consecutive eye drops • Some pts cannot tolerate ointments because of blurring of vision and the deposition on the eyelids (unacceptable cosmetic appearance and discomfort)
TIPS • Hence, prescribe drops during the day and ointments at night • Moreover, if necessary, drops should precede ointments because the latter impedes the absorption of the former
KINETICS: ADME • Topical drugs exert their effect by absorption via the cornea and conjunctival vessels • Excess drug is cleared via the lacrimal apparatus through the nasal mucosa and the nasopharynx ----- access to systemic circulation [and hence, systemic side effects] • Hence, instruct patients on manual nasolacrimal occlusion and eyelid closure for 1 to 2 min to decrease systemic absorption
Outline (based on PNDF) • Anti-infective agents • Anti-inflammatory agents - Steroids - NSAID’s • Diagnostic agents • Drugs used in glaucoma • Cholinergics • Beta-arenoceptor blocking drugs (Beta blockers) • Adrenergic agonsts • Prostglandin analogues • Carbonic anhydrase inhibitors • Hyperosmotic agents
Outline 6. Local anesthetics (not included) 7. Mydriatics and Cycloplegics (Anti-cholinergics)
Anti-Infective Agents: general • Avoid indiscriminate use of broad spectrum antibiotics, or • The use of antibiotics for excessively long periods of time • Caution on use of combined antibiotics & steroid preparations • RATIONAL PRESCRIBING: • To prevent emergence of resistant organisms • To avoid ADR’s (toxic eye reactions) • To avoid unnecessary expense
Anti-Infective Agents (general principles) • For maximal effect on ocular and periocular tissues, the properly dosaged and diluted IV antibiotic preparations may also be injected through the ff routes: subconjunctival, intracameral, intravitreal and retrobulbar areas
Chloramphenicol • Broad spectrum, bacteriostatic against most Gm (+), Gm (-) and anaerobic organisms • Resistance is increasing esp for hospital strains of staphylococci (50%) • High lipid solubility: good therapeutic evels in the aqueous humor • No route of admin can achieve good levels in the vitreous
Chloramphenicol • INDICATIONS: superficial infections of the eye caused by susceptible bacteria (used only when less toxic drugs are contraindicated or ineffective) • Local drug toxicity is rare • Consider systemic absorption ff topical ophtalmic application: “gray baby” syndrome, urticaria, allergic reactions (rash), bone marrow suppression (e.g. aplastic anemia) • Pregnancy Risk: C • Eye ointments (BID-TID) or drops (hourly or q 6hrs)
Erythromycin • Macrolide: gram positive cocci (staph, strep) and bacilli ; some gm (-) cocci (Neisseria) & bacilli (H. Influenzae, Moraxella, Chlamydiae, Treponema) • Recommended for prevention of neonatal ophthalmia • Pregnancy Risk Category: B
Erythromycin (cont) • Indications • Superficial infections of the eye caused by susceptible orgs • Adjunct to oral anti-infective therapy of Chlamydia infections (trachoma, inclusion conjunctivitis) • Prophylaxis of ophthalmia neonatorum from both gonococci and Chlamydia
Erythromycin (cont) • Dose: as eye ointment • Bacterial infections: OD to BID • Chlamydial ophtalmic infections: BID daily for 2 mos or BD for the first 5 days of each month for 6 mos • Prophylaxis of ophthalmia neonatorum: 1 cm ribbon of 0.5% ointment into each conjunctival sac immediately after birth: new tube for each neonate (single use)
Oxytetracycline • Bacteriostatic against gm (-) [Pseudomaonas aeruginosa, Entorobacteriacae] and gm (+) bacteria and against Rickettsia, Chlamydia, Mycoplasma, spirochetes, fungi & viruses • Penetrate ocular tissues better than other anti-infectives because of their high lipid solubility • Same indications as Erythromycin • Systemic absorption possible : serious dental & skeletal effects • Pregnancy risk category: D • Eye ointment
Gentamicin • Bactericidal for gm (-) aerobic organisms through bacterial ribosomal inhibition • Limited bioavailability: After topical application , much of the drug is bound to the iris and choroidal pigment • For superficial infections of the eye caused by susceptible orgs: Pseudomonas aeruginosa, E. Coli, Enterobacter, Klebsiell, Proteus, Serratia • Pregnancy risk: C • Ointment 2-3x/d, drops q1-4 hr
Tobramycin • Also an aminoglycoside against gm (-) orgs • Unlike gentamicin, has poor activity against Enterococcus and Mycobacterium • When inflammation is severe, there is a combined tobramycin + dexamethasone preparation (eye drops and ointment)
Framycetin • Aminoglycoside closely related to the neomycin group; bactericidal & active against both gm (+) and gm(-) bacteria found in superficial eye infections (staph, Pseudomonas, coliforms, and Pneumococci) • Treatment of local eye infections (Conjunctivitis, blepharitis) due to susceptible organisms; corneal abrasions, ulers and burns • Eye drops, 1 drop 3-4x/d
Aciclovir • Purine analog, 1st or 2nd gen antiviral specific for local treatment of Herpes simplex keratoconjunctivitis and varicella zoster viral infection • Highly effective effective viral DNA polymerase inhibitor in affected cells • For local treatment of HSV 1 and 2, varicella zoster infections affecting eye • Apply eye ointment to cover all lesions 5x/d for 14 days to start as soon as with signs & sx
Ganciclovir • Purine analog much like acyclovir but differs by an additional hydroxymethyl group on the side chain with wider spectrum of activity • HSV 1 and 2, Herpes varicella-zoster, EBV • Inhibits viral DNA synthesis by competitive inhibition of viral DNA polymerase and is incorporated into viral DNA as DNA chain terminator • Has potential to cause cancer, birth defects, azospermia (unlikely for topical but possible) • Pregnancy Risk category: C
Trifluridine • Thymidine analog which inhibits DNA polymerase and incorporates itself into DNA • Very effective against HSV 1 and 2,and vaccinia. Inhibits CMV and adenovirus in vitro • Precaution: may impair wound healing (post-op and thinned corneas) • Pregnancy risk category: C
Fusidate sodium (fusidic acid) • Antibiotic derived from Fusidium coccineum • Inhibits protein synthesis in bacteria, active against a wide range of gm (+) orgs esp staphy & Strep and some gm (-) orgs (pneumococus, Neisseria, Hemophilus, Moraxella, Corynebacterium) • No known cross-resistance with other antibiotics • Stable to bacterial beta-lactamases • Penetrates well into the aqueous humor • Drops suspension: 1 drop q 12 h
Ofloxacin • One of the 4 quinolones, bactericidal to a large number of gm (+) and gm (-) orgs through inhibition of DNA gyrase • For Staph aureus, H. influenzae, Pseudomonas aeruginosa, E. Coli, Klebsiella & enterobacteriacae, anerobes, legionella, Neisseria gonorrhea, Chlamydia trachomatis • Pregnancy risk category: C • Eye ointment, Eye drops solution
Povidone-iodine (topical) • Used as an epitheolytic agent causing destruction of corneal epithelium; • Does not remove viruses or enter live cells • Cocaine inactivates this agent; should not be used for corneal anesthesia • Indicated for superficial dendritic forms of herpes simplex keratitits when aciclovir and ganciclovir are not available • Used for peri-operative preparations of the conjunctiva and periocular skin
Anti-inflammatory Agents STEROIDAL NSAID
STEROIDAL • WARNING: Intake or application of corticosteroids to the eye may induce an attack of or aggravate open angle glaucoma • Inhibit inflammatory response of whatever cause: mechanical, chemical or immunologic agents • Inhibit redness, edema, exudation, capillary dilatation, fibroblastic proliferation and fibrin deposition, and cellular infiltration & migration of leukocytes and phagocytes, collagen deposition and cicatrization
Steroids • Stablize lysosomal membranes with prevention of release of kinins, inhibition of prostaglandin synthesis, and with chronic use decrease Ab production • Following instillation into the conjunctival sac, corticosteroids are absorbed into the aqueous humor and systemic absorption may occur
STEROIDS: Indications • Corneal & conjunctival inflammation such as allergic keratoconjunctivitis, episcleritis, immune viral interstitial keratitis • To decrease inflammation and rejection in corneal transplant • For uveitis, iritis and cyclitis, scleritis • Corneal, conjunctival, and scleral injuries from chemical, radiation and thermal burns • Treatment of post-op inflammation
Steroids: contraindications • Microbial, viral, fungal and tuberculous infections of the eye, unless these infections are controlled by appropriate chemotherapy, and use is under close supervision of a specialist • Precaution: some preparations contain sulfite, which may cause allergic reactions • Chronic use may cause corneal perforation • Example: prednisolone, dexamethasone drops suspension
Combination of Antibiotics & Steroids • Sulfacetamide + Prednisolone: eye drops suspension – 10% sulfacetamide + 0.25% prednisolone (as acetate), 5 mL bottle • Tobramycin + dexamethasone: • Eye Drops Suspension: 0.3% tobramycin + 0.1% dexamethasone, 5 mL bottle • Eye Ointment: 0.3% tobramycin + 0.1% dexamethasone, 3.5 g tube
NSAID’s • Used for local treatment of ocular inflammation without the disadvantages of steroids • E.g. diclofenac eye drops suspension • Reduces leukocyte accumulation and exudation into the chamber fluid • Has good penetration into the ant chamber • Re-epithelialization of the corneal epithelium is not inhibited by local diclofenac treatment
NSAID’s: Indications • Inhibition of intra-operative miosis during cataract surgery • Treatment of macular edema • Chronic conjunctivitis, ketaoconjunctivitis, keratitis, episcleritis • Painful post-traumatic conditions of the cornea and conjunctiva • Pre-op and in short- and long-term post-operative inflammatory process, to reduce ciliary and conjunctival injection • Corneal margin ulcers
NSAID’s: precautions • Use with caution on pts with known bleeding tendencies, or on medications that prolong bleeding • Pregnancy risk category: B • Generally well tolerated with only mild transient burning • Examples: Nepafenac Eye Suspension: 1 mg/mL, 5 mL bottle
DIAGNOSTIC AGENT: Fluorescein • Yellow water-soluble dibasic that produces an intense green fluorescence in alkaline medium • An indicator dye for the diagnosis of corneal epithelial defects or abrasions, & detection of foreign bodies; for testing the patency of the nasolacrimal drainage, fitting of contact lenses, etc • IV preparation is used to study the aqueous secretion of the ciliary body; for fluorescein angiography, and vitreous fluorophotometry
Pathophysiology of glaucoma • Increased intraocular pressure causes optic nerve damage, visual field deterioration and eventually blindness • Degree of damage depends on the level of the IOP and the chronicity of the conditio • Major therapeutic objective: reduce IOP urgently to arrest the damage to the optic nerve
Therapeutic options • Options for lowering IOP include • the use of topical or systemic medications, • laser trabeculoplasty, • surgery to improve outflow facility, and • cyclodestructive laser to reduce aqueous production.
Treatment of Glaucoma • Primary open-angle glaucoma is primarily treated medically, while angle closure glaucoma and congenital glaucoma are treated surgically, although short term drug therapy should be initiated to decrease intra-ocular pressure prior to surgery • IOP may be decreased by increasing the rate of outflow (drainage) of aqueous humor from the anterior chamber OR decreasing rate of production
CHOLINERGIC AGONISTS (miotics) • Parasympathomimetics which duplicate the effects of acetylcholine • Exerts effects on muscarinic receptors of the ciliary body stimulating the contraction of the longitudinal muscle fibers inserting to the scleral spur which then widens the valve-like pores of the trabecular meshwork facilitating outflow of aqueous humor • Possibly also a direct effect on the cholinergic receptors of the meshwork itself
CHOLINERGIC AGONISTS (miotics) • Pupilary constriction is NOT an imp’t factor for pressure reduction in open-angle glaucoma but is relevant in angle closure glaucoma • Constriction of pupil pulls the peripheral iris away from the trabecular meshwork • Other effects: vasodilatation of blood vessels of the conjunctiva, iris and ciliary body & inc permeability of blood-aqueous barrier leading to vascular congestion & ocular inflammation
CHOLINERGIC AGONISTS (miotics) • Contraindications: cause a breakdown of the blood-aqueous barrier- they are contraindicated in pts with acute ant chamber inflammation, pupillary block glaucoma, neovascular glaucoma • Caution in elderly (miosis leads to decrease in ambient light reception/dark adaptation). • Retinal detachment may rarely occur because of the drug-induced pull on the peripheral retina as the iris-lens diaphragm is pulled forward
Parasympathomimetics(cholinergic agents) *Values reported are relative change (%) from baseline (peak to trough effect). Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of glaucoma in the adult eye. Can J Ophthalmol 2009;44(Suppl 1):S1S93.