Download
1 / 1
10 likes | 150 Views
No127. Does allowing GPs direct access to CT KUB decrease emergency attendances or outpatient referrals?. Michael Vincent MBChB , David Brown MBChB , AFRCS(Ed ), FRCSEd ( Urol ), David Tulloch MBChB , FRCSEd ( urol )

E N D
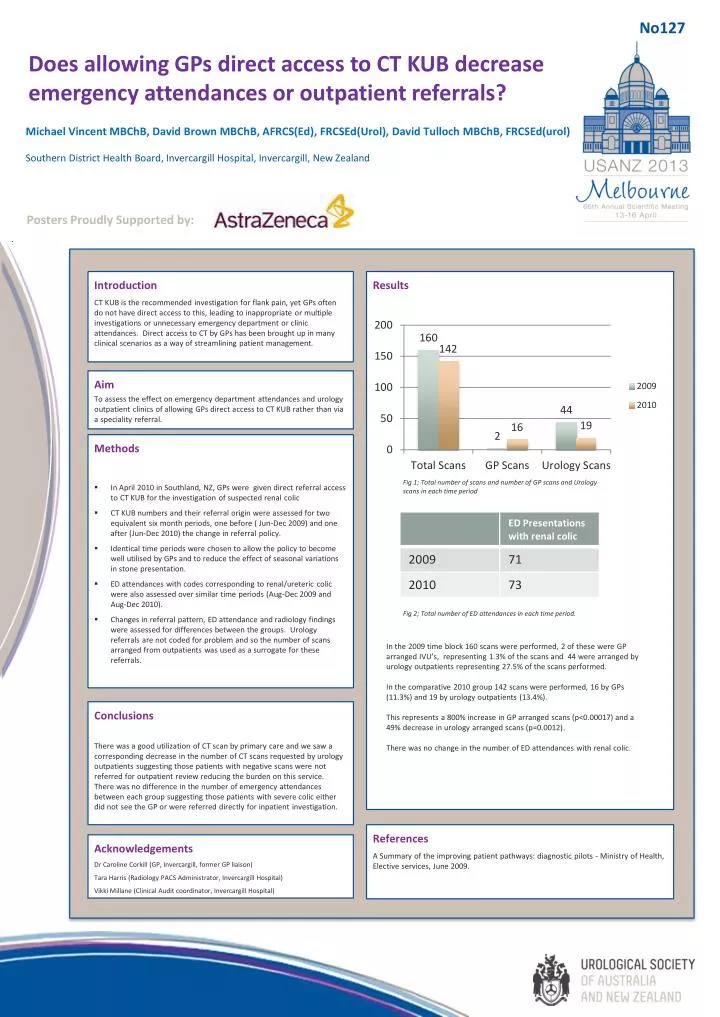
No127 Does allowing GPs direct access to CT KUB decrease emergency attendances or outpatient referrals? Michael Vincent MBChB, David Brown MBChB, AFRCS(Ed), FRCSEd(Urol), David Tulloch MBChB, FRCSEd(urol) Southern District Health Board, Invercargill Hospital, Invercargill, New Zealand Posters Proudly Supported by: Results Introduction CT KUB is the recommended investigation for flank pain, yet GPs often do not have direct access to this, leading to inappropriate or multiple investigations or unnecessary emergency department or clinic attendances. Direct access to CT by GPs has been brought up in many clinical scenarios as a way of streamlining patient management. Aim To assess the effect on emergency department attendances and urology outpatient clinics of allowing GPs direct access to CT KUB rather than via a speciality referral. • Methods • In April 2010 in Southland, NZ, GPs were given direct referral access to CT KUB for the investigation of suspected renal colic • CT KUB numbers and their referral origin were assessed for two equivalent six month periods, one before ( Jun-Dec 2009) and one after (Jun-Dec 2010) the change in referral policy. • Identical time periods were chosen to allow the policy to become well utilised by GPs and to reduce the effect of seasonal variations in stone presentation. • ED attendances with codes corresponding to renal/ureteric colic were also assessed over similar time periods (Aug-Dec 2009 and Aug-Dec 2010). • Changes in referral pattern, ED attendance and radiology findings were assessed for differences between the groups. Urology referrals are not coded for problem and so the number of scans arranged from outpatients was used as a surrogate for these referrals. Fig 1; Total number of scans and number of GP scans and Urology scans in each time period Fig 2; Total number of ED attendances in each time period. In the 2009 time block 160 scans were performed, 2 of these were GP arranged IVU’s, representing 1.3% of the scans and 44 were arranged by urology outpatients representing 27.5% of the scans performed. In the comparative 2010 group 142 scans were performed, 16 by GPs (11.3%) and 19 by urology outpatients (13.4%). This represents a 800% increase in GP arranged scans (p<0.00017) and a 49% decrease in urology arranged scans (p=0.0012). There was no change in the number of ED attendances with renal colic. Conclusions There was a good utilization of CT scan by primary care and we saw a corresponding decrease in the number of CT scans requested by urology outpatients suggesting those patients with negative scans were not referred for outpatient review reducing the burden on this service. There was no difference in the number of emergency attendances between each group suggesting those patients with severe colic either did not see the GP or were referred directly for inpatient investigation. References A Summary of the improving patient pathways: diagnostic pilots - Ministry of Health, Elective services, June 2009. Acknowledgements Dr Caroline Corkill (GP, Invercargill, former GP liaison) Tara Harris (Radiology PACS Administrator, Invercargill Hospital) Vikki Millane (Clinical Audit coordinator, Invercargill Hospital)






