Download

1 / 33
330 likes | 343 Views
Lining up for Joint Replacement. Panelists. Dr. Shelley Rahn, MassMutual Joe Furlong, RGA Reinsurance Elizabeth Roberge, MassMutual. Session Objectives. Anatomy of Knee Discuss OA/DJD process Underwriting Considerations Claim/Case Impact of Joint Replacement on disability and LTCi claims.

E N D
Panelists • Dr. Shelley Rahn, MassMutual • Joe Furlong, RGA Reinsurance • Elizabeth Roberge, MassMutual
Session Objectives Anatomy of Knee Discuss OA/DJD process Underwriting Considerations Claim/Case Impact of Joint Replacement on disability and LTCi claims
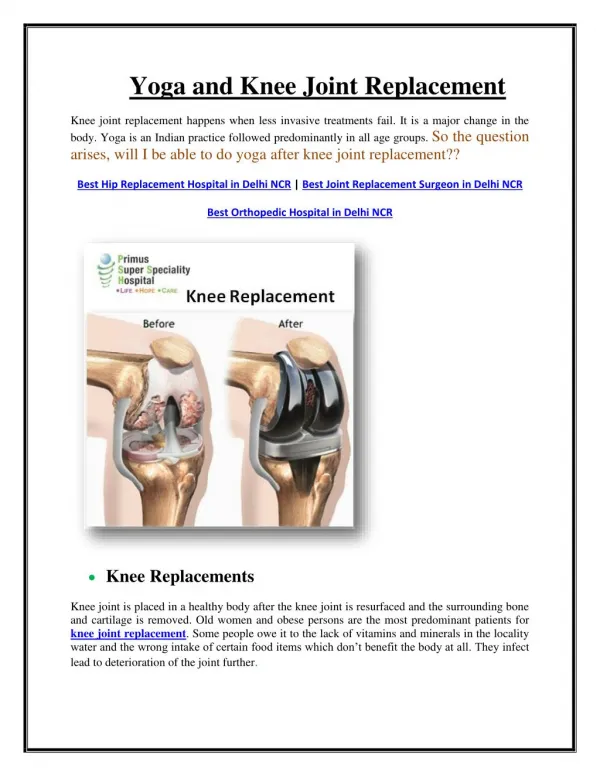
Osteoarthritis of the knee • Decrease in cartilage • Joint space narrowing • Bone on bone • Bone cysts • Bony spurs – osteophytes • Pain
Normal Knee Osteoarthritic Knee osteophytes Loose body A lateral radiograph of the knee is shown demonstrating significant OA of the patellofemoral compartment. There are prominent osteophytes (white arrows) and joint space narrowing (red arrow). Large ossified intra-articular loose bodies are also incidentally present (blue arrow).
Osteoarthritis • Primary • “wear and tear” • More likely to be bilateral • Other joints affected (hands, hips, back) • Secondary • Due to injury or trauma • May be unilateral
Risk of Developing Knee DJD Age - single biggest risk factor Obesity –increased impact with rising incidence of obesity Trauma Genetics Muscle weakness – especially quads Repetitive use – e.g., heavy lifting, bending
Knee Osteoarthritis Epidemiology • Highly prevalent among adults • Prevalence estimates vary widely by: • symptoms • X-ray – as high as 50% by age 65 • Strongly linked to late-life disability • Major cause of musculoskeletal pain
Underwriting Concerns Pain Presence and severity is single most important factor in shaping perception of disability Xrays with substantial osteoarthritic changes ^^risk of progression of symptoms Task modification often precedes self-reported task difficulty Quadriceps weakness:strongest single predictor of functional limitation Co-morbidities Depression/Anxiety Obesity
Post Knee replacement disability • Recovery – Gradual improvement over 3 months but ADL’s within first days to weeks to first month – Can improve up to one year post op • Pain • 10% to 34% after knee replacement at 3 years • Disability • Significantly less than preoperative • Affected by same factors as risk of progression • Motivation • Obesity • Quadriceps strength • Life expectancy of the replacement – now up to 20 years • Can just replace the liner without needing complete new joint
Claims The challenge at claim time is to: Manage the expectations of the claimant and family. Determine expected length of ADL deficiency. Determine when recovery has been achieved and the Benefit Triggers are no longer being satisfied.
TQ vs. Non-TQ There is a good chance of qualifying for benefits on pre-HIPAA and other Non-TQ Policies. Few claims will satisfy the Chronically Ill Individual requirement on TQ Policies but it can happen, especially if there are complications.
Case Study What can go wrong – a challenging case study
Case Demographics At policy issue; 44 yo male 6’ 205 lbs Meat Department Manager for a large grocery store chain Benign medical history, essential HTN controlled with 100 mg Tenormin
At time of claim 59 yo male 6’ 260 lbs History of severe constant bilateral knee pain for the past several years On examination moderate crepitance and minimal varus deformity Range of motion is 0 to 135 º Weight bearing X-ray examination shows severe degenerative joint disease
At time of claim 59 yo male 6’ 260 lbs History of severe constant bilateral knee pain for the past several years On examination moderate crepitance and minimal varus deformity Range of motion is 0 to 135 º Weight bearing X-ray examination shows severe degenerative joint disease
In the knees, primary OA predominately involves the medial tibiofemoral and patellofemoral compartments. The asymmetric medial joint space loss (white arrow) causes a varus deformity on standing radiographs. A large osteophyte classically forms on the medial tibial articular margin (red arrow). Subchondral sclerosis and cyst formation may also be found.
Treatment Plan Insured failed to benefit from non operative treatment Bilateral total knee replacements were scheduled for January 18 2011
Surgery and Recovery 01/18/11 bi lateral total knee replacements 02/04/11 wound healing, sensory and motor without deficit, knee range of motion 50-90º; patient walking with a moderate antalgic gait with the aid of a walker 2/05/11 PT going well until yesterday, both knees stiffening. Mild erythema of the right knee, range of motion 5-80º
Complications 03/04/11 Bilateral closed knee manipulation 5 weeks of physical therapy, Keflex 500 mg 4x day for 10 days. Patient to advance physical activities as tolerated. 03/18/11 No erythema, warmth or effusion. Gait is within normal limits. Knee range of motion 5-105º Physical therapy 3x week, for six weeks. Antibiotic prophylaxis and DVT prophylaxis. Advance activities as tolerated.
Complications Continued 4/1/2011 Moderate effusion on both knees, worse on left. Left knee range of motion 0-91º, right 0-98º. Additional physical therapy prescribed; patient remains dependent on walker and needs assistance of HHA. 5/13/2011 2nd bilateral knee closed manipulation 7/20/11 severe contracture of the left knee
Complications Continued 7/29/11 left knee arthroscopy, debridement of arthrofibrosis, lateral patellar retinacular release 9/9/11 post op visit, minimal pain relief noted, 8 weeks of PT prescribed
January 2012 01/10/12 Patient continues to require a walker and assistance of HHA. PET scans reveals infected bilateral knee arthroplasties. New surgical consult, recommendation for 2 stage bi lateral procedures, possibly 4 separate surgeries for antibiotic spacers followed by re-implantation of right, then left. Surgeries and recovery expected to last 12 months. Patient may not recover to pre morbid level of functioning.
Physical Therapy Notes What should we be looking at to determine progress toward recovery? How are they deciphered?
Claim Management Frequent contact with the claimant is key. “How did PT go today? How is the caregiver helping you?” The claimant should have the expectation that they will recover and that at some point, care will no longer be required and benefits will end. Managing these claims properly will take time but it will be worth it in the long run.
Closing a Claim How is this communicated to the claimant? Should not be a surprise. Prior communication with the claimant is key to success here, assuming you have set the appropriate expectation.
Knee Replacements: Summary • Generally, should not trigger a claim on a TQ policy • Premorbid condition is often worse than eventual post op • Long term complications are infrequent • Managing the claim is key