Download
1 / 15
150 likes | 298 Views
Ebola Viral Disease. October 21, 2014. O verview. Historical perspective Current epidemic update OSUWMC preparedness Signage and marketing Screening Isolation activation Inpatient management Staff education and training; simulations Challenges. Challenges.

E N D
Ebola Viral Disease October 21, 2014
Overview • Historical perspective • Current epidemic update • OSUWMC preparedness • Signage and marketing • Screening • Isolation activation • Inpatient management • Staff education and training; simulations • Challenges
Challenges • Balancing preparedness and informative education with alarmism • Forced isolation/treatment • Global presence of our university community • Dynamic nature of the epidemic • Changing protocols • Other problems to not forget…. • Enterovirus D68, Influenza
Ebola Epidemiology • Acute infection starts as a non-specific febrile illness • Fever (>100.4), severe headache, muscle pain, malaise; progression to include GI symptoms (diarrhea and vomiting) • Symptoms may appear 2-21 days after exposure • 8-10 day window the most common • Significant dehydration and electrolyte disturbances • Small vessel involvement • Increased permeability due to cellular damage • Multi-organ system failure • Hemorrhage may develop in the second week • Poor prognosis associated with shock, encephalopathy, extensive hemorrhage Jay Varkey, MD; Emory University Hospital
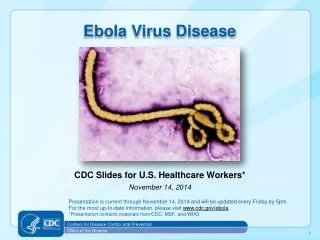
Ebola Historical Perspective Jay Varkey, MD; Emory University Hospital • Family Filoviridae • Two genera: marburgvirus and ebolavirus • Enveloped RNA virus • Five subtypes of Ebola virus • Zaire (EBOV) • Sudan (SUDV) • Tai Forest (TAFV) • Bundibugyo (BDBV) • Reston (RESTV) • No vaccines/treatments approved for humans • Case-fatality rates of up to 90% in African settings
Ebola Historical Perspective Jay Varkey, MD; Emory University Hospital • 1976: Simultaneous outbreaks in Zaire (now DRC) & Sudan • Zaire: 318 cases and 280 deaths (88% mortality) • Sudan: 284 cases and 151 deaths (53% mortality) • 1976 & 1979: Small-to-midsize outbreaks Central Africa • 1995: Large outbreak in Kikwit (DRC) • 315 cases (81% mortality) • Since 2000: Near-yearly outbreaks in Gabon, DRC or Republic of Congo • 2000-2001: Largest outbreak on record (Sudan) • 425 cases (53% mortality)
Current EVD Epidemic • West African outbreak limited to: • Guinea: 1519 cases / 862 deaths • Liberia: 4249 cases / 2484 deaths • Sierra Leone: 3410 cases / 1200 deaths • Total: 9178 cases / 4546 deaths • Senegal (8/29/14) and Nigeria (9/5/14) no longer considered at risk • Early August 2014 – first health care workers brought from West Africa to Emory University Hospital • Other individuals brought from West Africa since then • September 30, 2014 – first case diagnosed in the US (Dallas) of a Liberian man traveling to the US • Patient passed away October 8, 2014 www.cdc.gov and Fox News
Current EVD Epidemic • Two nurses at Dallas hospital have tested positive for Ebola (October 10th and October 14th) • Second nurse traveled through NE Ohio from 10/10-10/13 • Over 100 people in NE Ohio on quarantine/isolation or monitoring of temperatures • Risk points of when a health care worker can most commonly become infected: • From exposure to body fluids during patient care • From error during doffing of PPE • From time when patient is intubated or during certain procedures due to increased aerosolization of secretions www.cdc.gov and Fox News
EVD Preparedness at OSUWMC • Both UH and UHE ED’s need to be prepared for walk-ins and EMS traffic • Volunteer team designated for inpatient care • Medical Team • Nursing • RT/team • Six hours of training in three two-hour phases • “Buddy System” for PPE • Point of Care testing equipment for in-room use for routine labs • EVS, solid and liquid waste plans developed
EVD Preparedness at OSUWMC • All patients planned to be admitted to 5 Ross – this may change after mid-December when old James available • Will have a donning/doffing room adjacent to each room • Entry restricted to assigned care team with log • 2 nurses per patient – one inside/one outside • If critically ill, consider two inside/one outside • Team huddle including Critical Event Officer and senior clinical leaders two times per day • No transport outside room unless approved by the Critical Event Officer • All deviations to SOP’s need to be approved by Critical Event Officer prior to implementation
EVD Preparedness at OSUWMC • Collaboration between the CMO’s of Franklin County Hospitals, Columbus Public Health and COTS • Outreach to regional hospital leadership and MedCare ambulance service • “Secret shopper” simulations • Three+ have been completed • Screening questions in outpatient IHIS workflows with BPA that fires if screen positive to alert rest of care team • Working closely with University officials on how this will affect the rest of campus
Challenges • Balancing preparedness and informative education with alarmism • Forced isolation/treatment • Global presence of our university community • Dynamic nature of the epidemic • Changing protocols • Other problems to not forget…. • Enterovirus D68, Influenza
Special thanks to Drs. Naeem Ali, Julie Mangino, and Christina Liscynesky for resources and data