Download
1 / 48
480 likes | 673 Views
Population Health Readiness Self-Assessment NC Critical Access Hospital Network Regional Meeting May 22, 2019. Financial Indicators. Goals for Today. To stimulate your thinking regarding transformational shift from the current “sick care” to future “health care” delivery model

E N D
Population Health • Readiness Self-Assessment • NC Critical Access Hospital Network Regional Meeting • May 22, 2019 • Financial Indicators
Goals for Today • To stimulate your thinking regarding transformational shiftfrom the current “sick care” to future “health care” delivery model • To share your self-assessment readiness level for navigating towards population health delivery model • To encourage proactive planning and engagement related to population health positioning
Project Summary • Online survey • Available to all NC CAHs • One response per hospital • Administered in 2017 • 16 CAHs participated • Administered in 2019 • 11 CAHs participated
Transition Framework FFS PBPS PHASE I PHASE II PHASE III Implement Improve quality and efficiency Implement DELIVERY SYSTEM TRANSFORMATION Align primary care providers Plan Implement Rationalize service network Strategize Plan • Data analytics • Care management • Evidence-based protocols • Payer and network contracting • Value attribution • Plan design • Risk management • Value-based credentialing Population Based Health System POPULATION HEALTH SYSTEM CREATION Implement Full-risk payment Plan Strategize Implement PAYMENT SYSTEM TRANSFORMATION Shared saving payments Plan ESHP & FFS payment with incentives Implement
Hospital-centric “Sick” Care Model LTC Primary Care HHA Hospital ASC / Dx Centers Urgent Care Retail Pharmacy • Diagnosis and treatment focus with acute care emphasis • Hospital as hub with fragmented care coordination • Limited informatics interconnectedness • Payment model fosters incentive to drive / capture episodes
Emergence of a System of “Health” Care Acute Care Hospital Community-Based Care Post-Acute Care Skilled Nursing Facility Retail / Pharmacy Acuity Source: Sg2 • Wellness and prevention focus • Hospital is not sole destination setting for highest acuity patients • Team-based care coordination across continuum • Interconnected informatics / telehealth platform • Payment model based on aligned incentives and shared risk with goal of value and “health” creation
Where to focus? Operating Efficiencies Care Management Population Health Quality and Engagement Informatics/Analytics Business Practices PCMH Delivery System Primary Care Networks Employee Health Plans Payment System Health System Alignment Transitional Payment Models Specialists Physician Leadership Facilities Governance Culture Change Management
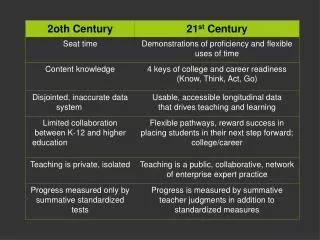
What to change to? Now Future A B Reform Shaky Bridge No Transition Because of the complexity and uncertainty facing hospitals, for many CEOs the most prudent and comfortable strategy is also the least disruptive and potentially controversial strategy – to resist taking bold steps. Full Transition The fundamental role of a hospital is changing rapidly – away from a physical location where patient care is provided to the centerpiece of a highly integrated rural health system for residents of a rural community. To be successful, health systems of the future will assume financial, quality, satisfaction and health status accountability for its community and will take on a new set of strategies, philosophies and performance metrics.
Fundamental Changes Now Future A B Patients Hospitals and Medical Staffs Revenue Centers Private Payers Primary Care Providers Productivity Bonuses FFS Volume Growth Charge Masters Expand to be Flip 180 into Lose relevance to Mature into Is supplanted by Evolve into Are viewed as Become $21m Service Line Leaders Cost Centers Value Bonuses Cost Masters Community Health Systems Full-Risk Aggregated Lives Competing Providers Price-sensitive Purchasers
Group Questions • Are you discussing the transition to Population Based Payment with key stakeholder groups (e.g. Board, Medical Staff, Hospital Associates and Community)
Self Evaluation Scale • Each category has a 5-point scale 0 1 2 3 4 A 1 2 3 B No Transition Rural delivery systems that are scored as “A” have made no transition progress. For example, a health system that has no risk-based contracts and does not participate in quality and patient satisfaction public reporting. Initial Steps Rural delivery systems that are scored as “1” have made some incremental Transition steps in targeted areas. For example, a health system that has invested in information technology and has its medical staff using CPOE. Mid Range Rural delivery systems that are scored as “2” have made several Transitional steps and have plans for taking more steps. For example, a health system that has implemented Patent Centered Medical Homes and that have hired dedicated care managers. Major Progress Rural delivery systems that are scored as “3” have made significant Transition progress. For example, a health system that has assumed risk-based contracts for private payers and has advanced informatics capabilities for monitoring cost and quality performance. Full Transition Rural delivery systems that are scored as “B” have largely made the full Transition. For example, a health system that has developed its own insurance products and successfully assumes full-risk contracts and has a fully-integrated delivery system.
2017 Results Summary by Cluster FH Montgomery Highlands-Cashiers Vidant Chowan Transylvania Murphy Pender Swain St. Luke’s Dosher Ashe Cannon Chatham Angel Bladen Blue Ridge Alleghany
2019 Results Summary by Cluster FH Montgomery Vidant Chowan The Outer Banks Dosher Murphy Pender Swain Cannon Chatham Bladen Alleghany
Delivery: Operations • Operational processes such as cost management, staffing to volumes, point of service collections, seamless scheduling, transitions of care and information flow across the continuum. A 1 2 3 B Future -- Full Transition Clinical and business operations are “efficient” and tightly integrated resulting in easy access to care, low wait times, minimal re-work and availability of information at all care points. All leaders and managers understand the importance of unit cost management, maintaining appropriate patient services, effective billing and collections, including at the point of service, and exploring new sources of revenue within an efficient cost structure.
Delivery: Operations The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Delivery: Quality and Engagement • Clinical processes and outcomes combined with patient satisfaction and confidence represent publicly-available and well-known evidence of the quality of care available locally. A 1 2 3 B Future -- Full Transition The rural delivery system participates in public reporting programs (State, Federal and Private), monitors provider performance using industry-standard metrics, and demonstrates better quality than its local competitors. The quality of care is well known throughout the community and results in a high degree of confidence for using services locally, with limited out migration. Quality is recognized as “everyone’s job” and is visibly supported by leadership.
Delivery: Quality and Engagement The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Delivery: Primary Care Alignment • The community has access to a full complement of physicians and advance practitioners who provide local access to high quality care. A 1 2 3 B Future -- Full Transition The rural delivery system’s population has access to local primary care services (whether through employed PCPs, independent practices, rural health clinics, and/or FQHCs). This provider network has shared incentives that are aligned with the health system’s mission and strategy incorporation functional, contractual and governance connections. Employed primary care is supported with effective practice management services that help practitioners grow and manage their local panel size and address primary care needs efficiently.
Delivery: Primary Care Alignment The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Delivery: Specialty Alignment • The full complement of specialty services available to the community provided in coordination with primary care and delivered locally whenever feasible. A 1 2 3 B Future -- Full Transition The rural delivery system evaluates patient demand for services using informatics and recruits specialists to match population-based supply with demand. Primary care to specialist relationships are developed and monitored based on the health system’s clinical standards. Specialists actively work with primary care providers to coordinate across the continuum of patient needs, with services always provided locally when clinically appropriate.
Delivery: Specialty Alignment The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Delivery: Facilities • Strategic investment in bricks and mortar that results in a highly efficient and patient friendly experience. Inpatient capacity is sized to the needs of the population and ambulatory services have proper adjacencies and patient convenience. A 1 2 3 B Future -- Full Transition Investments in sites, buildings and equipment are right-sized and provide the rural delivery system optimal flexibility to adapt to changing requirements. Facilities enable the rural system strategy and support efficient operations, high quality and the transition of care from inpatient to ambulatory settings. Decision-making criteria take into account expected changes in health service utilization, system integration, and payment trends.
Delivery: Facilities The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Delivery: Health System Alignment • The rural health delivery system uses a proactive strategy to develop its affiliation strategy to enhance the sustainability of service availability and rationalize services across the spectrum of care. A 1 2 3 B Future -- Full Transition The rural delivery system has a regional alignment strategy that includes other providers and/or payers to ensure patients receive all necessary services at the optimal time, place, quality, and cost. The rural system’s partners recognize the value of the rural delivery system, have processes to enhance it, and attribute value back to the primary care site(s). The scale provided through its partnership(s) enable the rural system to access transitional and population-based payment approaches that enhance sustainability.
Delivery: Health System Alignment The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Group Questions Do you have a transition plan for Population Health? If so, please share what progress has been made.
Population Health: Care Management • Community and patient engagement through outreach, education and relationship development to ensure access to care, a reduction in unnecessary services, and improved population health status. A 1 2 3 B Future -- Full Transition The rural delivery system employs and/or contracts with dedicated care managers who partner with the community’s primary care providers to coordinate patient care across the entire health care system. Care managers actively monitor overall patient health and wellness and are evaluated on their ability to minimize unnecessary care, improve health status, and manage total costs by payer.
Population Health: Care Management The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Population Health: Patient Centered Medical Home (PCMH) • The culture, values, provider base and clinical infrastructure are recognized in fully-certified Patient Centered Medical Homes. A 1 2 3 B Future -- Full Transition The rural health system has led or facilitated the development of PCP-based Patient Centered Medical Homes and has established value-based payment models with commercial payers to fund care coordination, reduce total patient costs, implement preventive care initiatives, support community-based patient engagement, and provide financial rewards for achieving improved patient outcomes at lower PMPM cost.
Population Health: Patient Centered Medical Home (PCMH) The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Population Health: Informatics/Analytics • The aggregation of disparate data sources (across both internal systems and external warehouses) to enable strategic, market, clinical and operational analysis and use of the data to create high performing systems. A 1 2 3 B Future -- Full Transition The rural delivery system has a culture that embraces data and analytics, understands the value of measurement, and uses an array of provider scorecards to evaluate cost, quality, and patient engagement while leveraging public and private data to evaluate internal and external performance in the market. A key objective is to receive and manage claims-level data to enable PMPM analysis and risk management for population-based contracting strategies and to use the data for attributing performance to where it is created in the system.
Population Health: Informatics/Analytics The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Culture: Physician Leadership • Aligned medical staff buy-into and actively lead, support and/or reinforce health system delivery transformation. A 1 2 3 B Future -- Full Transition The rural delivery system’s medical staff and regional providers are closely aligned with the organization’s mission and strategy, collaborate well as a team and actively embrace system-wide change to preserve the organization’s mission and to fulfill the overarching goal of optimal health outcomes for the community. Key members of the medical staff have assumed leadership roles in the organization and have buy-in from other members of the medical staff.
Culture: Physician Leadership The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Culture: Governance • Hospital trustees understand the urgency and complexity surrounding healthcare transformation and play a fiduciary role in fostering organizational change. A 1 2 3 B Future -- Full Transition The rural delivery system’s Trustees are well educated on the future challenges and impending changes, have endorsed and are monitoring a formal strategy to prepare for the future and are equipped to facilitate and support the management team’s decision making process. Trustees understand and execute their fiduciary responsibility consistently.
Culture: Governance The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Culture: Change Management • Hospital employees, executives, medical staff and trustees recognize the importance of culture and learner styles on the organization’s ability to affect change. A 1 2 3 B Future -- Full Transition Change is viewed as a natural, positive phenomenon that signals the vitality of the rural health system. Staff, physicians and Trustees all embrace the opportunity to improve processes and to grow in ways that are respectful, effective, equitable and efficient. Communication across the system flows seamlessly (vertically and horizontally) based on intentional Organizational Design principles that balance incentives, performance monitoring and decision rights. Growth occurs intentionally with empowered managers who operate as “pitchers” vs. “catchers”.
Culture: Change Management The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Payment: Employee Health Plans • Comprehensive, self-funded insurance product for the health system’s employees and their family members. A 1 2 3 B Future -- Full Transition In a fully transitioned environment (Option B below), through aggregation of insured lives, the rural health system maintains a full-service, self-funded employee health plan that manages costs effectively and provides incentives for health and wellness. The rural delivery plan is scalable to other local and/or regional public and private employers.
Payment: Employee Health Plans The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Payment: Transitional Payment Models • Value-Based and Population-Health-oriented contracting with third-party payers. A 1 2 3 B Future -- Full Transition In a fully transitioned environment, the rural delivery system is viewed as a leader in developing and implementing novel (and advantageous) reimbursement models based on value (cost and quality) and other parameters specific to the health system. Payer contracting capabilities are viewed as a strategic advantage rather than a process where the health system plays a subordinate role to third-party payers. Short term opportunities include public and commercial Shared Savings programs.
Payment: Transitional Payment Models The Outer Banks Vidant Chowan FH Montgomery Dosher Swain Cannon Chatham Bladen Murphy Alleghany Pender
Transition Timing • Late Starters • Sequential • First Movers • Competitors and potential collaborators have already made the transition and view your organization as a liability • Modifying the wrong strike points in the wrong order creating organizational tension and disruption • Implementing changes to delivery system without harmonizing with payment system • Risks • Difficult decisions and changes are implemented on the front end creating time for well-informed strategic decision making and adjustments • Learn from other organizations that have made modifications and use that knowledge to foster success • Deliberate, scheduled process for transitioning the most ready strike points at the best time • Rewards
Addressing your Bottlenecks Operating Efficiencies Assess, benchmark and develop focused action plans Value and Engagement Maximize performance on public reporting programs Care Management Employ or contract for care coordinators Business Practices Ensure high performance revenue cycle management Facilities Drive out unnecessary PP&E fixed costs Health System Alignment Define criteria and monitoring systems for collaborators Physician Leadership Identify, empower and support physician leaders Change Management Educate people and invest in processes to facilitate change
Group Questions • What actions will you take following this meeting to better prepare your organization for the transition to Population Based payment?
Financial Indicators Questions? 1685 Congress St. Suite 202 Portland, Maine 04102 (207) 221-8250 www.stroudwater.com