Download
1 / 12
120 likes | 311 Views
S urveillance of HIV in most-at-risk populations in the Middle East and North Africa : Recent Development s. Dr Gabriele Riedner, WHO EMRO On behalf of the Regional UN Working Group on HIV surveillance. The presentation - outline.

E N D
Surveillance of HIV in most-at-risk populations in theMiddle East and North Africa: Recent Developments Dr Gabriele Riedner, WHO EMRO On behalf of the Regional UN Working Group on HIV surveillance
The presentation - outline • Epidemiological evidence on HIV in most-at-risk populations: status in 2005 • The joint strategy of regional partner agencies • Epidemiological evidence today • Lessons learnt • The way forward
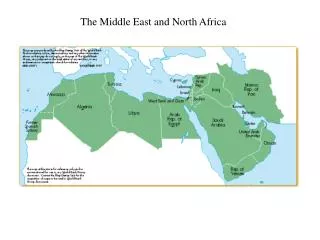
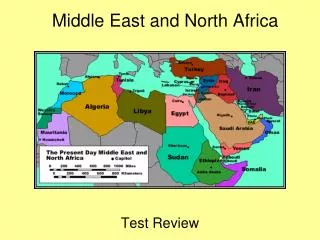
2005: The HIV epidemic situation among most-at-risk populations is largely unknown Regional context: Limited evidence and low visibility of the HIV epidemic; high stigma; prosecution of MSM, SW, IDU Situation assessments among IDU, MSM and SW initiated in 7 countries findings: low HIV knowledge and awareness; high risk behaviours Available data on HIV in most-at-risk populations stem from (largely non-systematic) testing in institutional settings showing elevated HIV prevalence (see next slide)
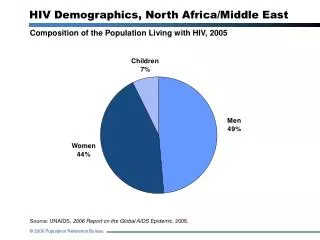
Summary of 44.6 million HIV tests from country reports provided to WHO (1989-2007)
Joint strategy of regional partner agencies* • Advocacy for “Knowing the Epidemic” (and access to prevention and care services for populations at risk) • Technical guidance and training materials addressing region-specific issues • Major investment in training of experts within the Region on survey methodologies • Regional “Knowledge Hubs” (2009: Kerman UMS) • Technical support to and funding of surveys *UNAIDS , WHO, WB + collaboration with UNODC, KH Zagreb, CDC, UCSF, FHI,
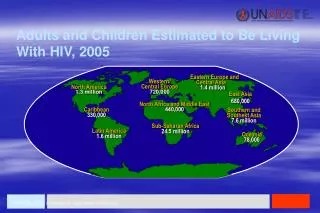
2008: Knowledge of the HIV epidemic situation has substantially increased 10 countries studied HIV prevalence + behaviours of most-at-risk populations; 7 countries used RDS and/or TLS. Other systematic sampling method: RDS/TLS use: SW IDU MSM SW and/or MSM and/or IDU
HIV prevalence among most-at-risk populations (surveys using RDS/TLS) • IDU (and DU): • Iran ≤ 25%; Iran (DU) 6.3%); Pakistan ≤ 26%; • Egypt 0.6%; Lebanon 0%; • MSM: • Lebanon 3.6%; Egypt 6.2%; Pakistan MSW ≤1.5% • Sudan and Iran: not yet available • SW: • Lebanon 0.7%; Yemen 1.3%; Pakistan 0.2%; • Sudan and Somalia: not yet available
Some lessons learnt • Careful involvement of government and community leaders at national and local levels essential; Due attention to stake-holders’ concerns to ensure support and to prevent interference of authorities during surveys; • Thorough pre-surveillance assessment! Know the population; explore incentives; Sufficient resources and time to be allocated; • Populations can be small and prevalence low: implications on sample size, budget/time/feasibility
Lessons learnt (ctd.) • Due to high stigma and fear of prosecution SWs and MSM are very hidden and network sizes can be very small. Refusals may occur frequently. • Interaction between researchers (from NGOs, academic institutions, NAPs) and populations studied led to • deeper understanding and less stigmatizing attitude towards the populations studied • knowledge of and demand for services by participants • thus laying a good foundation for interventions after the study. • Data dissemination strategy is a major challenge.
The way forward: • Sustain advocacy, local capacity building, technical support and inter-country experience exchange – it makes a difference! • Emphasize surveillance system development; • and be vigilant of potential HIV risk scenarios outside the classical core – bridging group scenario; • Develop joint (UN and partners) strategy to promote enabling environment